Renal oncocytoma
| Renal oncocytoma | |
|---|---|
| Diagnosis in short | |
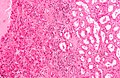
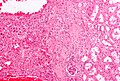
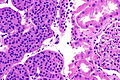
 Renal oncocytoma (left of image) and normal kidney (right of image). Kidney biopsy. H&E stain. | |
|
| |
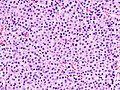
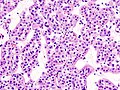
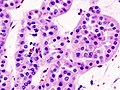
| LM | abundant eosinophilic cytoplasm - slightly granular, cells arranged in nests, nuclei uniform and round without significant pleomorphism |
| LM DDx | chromophobe renal cell carcinoma eosinophilic variant, clear cell renal cell carcinoma eosinophilic variant, papillary renal cell carcinoma oncocytic variant, tubulocystic carcinoma of the kidney, other renal tumours with eosinophilic cytoplasm |
| Stains | Hale's colloidal iron -ve |
| IHC | CK7 -ve/cytoplasmic +ve, PAX2 +ve |
| EM | abundant mitochondria |
| Gross | mass, mahogany brown +/- central scar |
| Grossing notes | partial nephrectomy grossing, total nephrectomy for tumour grossing |
| Site | kidney - see kidney tumours |
|
| |
| Clinical history | often incidentally discovered mass |
| Radiology | renal mass with central scar (classic) |
| Prognosis | benign |
| Clin. DDx | other kidney tumours |
Renal oncocytoma is a benign kidney tumour that is removed to exclude malignancy.
General
- Can be difficult to distinguish radiologically from RCC (chromophobe subtype).
- ... and pathologists occasionally struggle like the radiologists.
- Benign tumour - the reason it is excised is... one cannot be certain it isn't a RCC.
Gross
- Mass, mahogany brown.
- Well circumscribed.
- 1/3 have a characteristic central scar.[1]
Image

Renal oncocytoma with central scar. (WP)

Microscopic
Features:
- Eosinophilic cytoplasm - slightly granular key feature.
- Cells arranged in nests.
- Nuclei uniform and round.[1]
- Slightly enlarged nuclei, but no significant pleomorphism (size variation) - important.
Notes:
- May look like eosinophilic variant of chromophobe RCC -- this is the main DDx.
- A comparison based on histomorphology: Tabular comparison between ChRCC & oncocytoma.
- Oncocytoma typically has: no perinuclear clearing, no raisinoid nuclei, rare or no binucleation.
- A comparison based on histomorphology: Tabular comparison between ChRCC & oncocytoma.
- May have - according to Trpkov et al.:[2]
- Vascular invasion ~4% of cases.
- Chromophobe-like area <5% of neoplasm ~12% of cases.
- Focal clear cell changes ~15% of cases.
- Hemorrhage.
DDx:
- Chromophobe renal cell carcinoma, eosinophilic variant.
- Succinate dehydrogenase-deficient renal cell carcinoma - emerging entity as per Vancouver classification - classically has a flocculent cytoplasm, may have oncocytoma-like areas.
- Papillary renal cell carcinoma, oncocytic variant.
- Renal hybrid oncocytic/chromophobe tumour.
- Clear cell renal cell carcinoma, eosinophilic variant.
- Tubulocystic carcinoma of the kidney.
- Other renal tumours with eosinophilic cytoplasm.
Images
Case 1
Oncocytoma. (WC/KGH)
Oncocytoma. (WC/KGH)
Oncocytoma. (WC/KGH)
.jpg)
.jpg)
.jpg)
Case 2
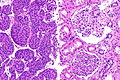
Oncocytoma - high mag. (WC/Nephron)
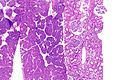
Oncocytoma - intermed. mag. (WC/Nephron)

Oncocytoma - low mag. (WC/Nephron)



Case 3
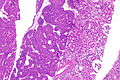
Oncocytoma - low mag. (WC/Nephron)
Oncocytoma - low mag. (WC/Nephron)
Oncocytoma - intermed. mag. (WC/Nephron)
Oncocytoma - high mag. (WC/Nephron)



Stains
- Hale's colloidal iron -ve.
- ChRCC +ve (blue granular cytoplasmic).
IHC
- CK7 -ve[3]/+ve (cytoplasmic) .
- Chromophobe renal cell carcinoma = cell membrane +ve.
Others:
- PAX8 +ve.[4]
- CD117 +ve.[5]
- ChRCC also +ve.
- CD10 -ve/+ve.
- Amylase α-1A +ve.[6]
- PAX2 +ve.[7]
- Oncocytoma 20 of 23 +ve versus ChRCC 1 of 11 +ve.
A panel:
- CK7, PAX8, CD117, CD10, Mueller-Mowry stain.
Sign out
Biopsy
KIDNEY MASS, RIGHT, CORE BIOPSY: - RENAL TUMOUR WITH ONCOCYTIC CYTOPLASM, FAVOUR ONCOCYTOMA. COMMENT: The tumour is CK7 negative and Hale's colloidal iron negative.
Micro
The sections show a tumour with cells arranged in nests. The tumour cells have abundant eosinophilic cytoplasm. The tumour cell nuclei are predominantly round. No perinuclear halos are apparent. Binucleation is not common. No zonal necrosis is identified. Focally, tumour nests are spaced reminiscent of an archipelago. Mitoses are not apparent. The tumour is moderately circumscribed.
A small amount of renal parenchyma is present. No definite glomeruli are identified. No significant interstitial fibrosis is present. No inflammation is apparent.
Resection
PORTION OF KIDNEY, LEFT, PARTIAL NEPHRECTOMY: - ONCOCYTOMA. COMMENT: The tumour is CK7 negative and Hale's colloidal iron negative.
Micro
The sections show a tumour with cells arranged in nests. The tumour cells have abundant eosinophilic cytoplasm. The tumour cell nuclei are round and have round nucleoli. No perinuclear halos are apparent. Binucleation is not common. No zonal necrosis is identified. Focally, tumour nests are spaced reminiscent of an archipelago. Mitoses are not apparent. The tumour is moderately circumscribed and is completely excised in the planes of section.
The thin rim of renal parenchyma has no apparent glomerular pathology on the H&E stained sections. Mild-to-moderate atherosclerosis is present. Mild arteriolar hyalinization is identified.
The Hale's colloidal iron stain is negative in the tumour. A CK7 immunostain has very rare positive cells within the tumour; this is interpreted overall as negative.
See also
References
- ↑ 1.0 1.1 Zhou, Ming; Magi-Galluzzi, Cristina (2006). Genitourinary Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 302. ISBN 978-0443066771.
- ↑ Trpkov, K.; Yilmaz, A.; Uzer, D.; Dishongh, KM.; Quick, CM.; Bismar, TA.; Gokden, N. (Dec 2010). "Renal oncocytoma revisited: a clinicopathological study of 109 cases with emphasis on problematic diagnostic features.". Histopathology 57 (6): 893-906. doi:10.1111/j.1365-2559.2010.03726.x. PMID 21166703.
- ↑ Liu, L.; Qian, J.; Singh, H.; Meiers, I.; Zhou, X.; Bostwick, DG. (Aug 2007). "Immunohistochemical analysis of chromophobe renal cell carcinoma, renal oncocytoma, and clear cell carcinoma: an optimal and practical panel for differential diagnosis.". Arch Pathol Lab Med 131 (8): 1290-7. doi:10.1043/1543-2165(2007)131[1290:IAOCRC]2.0.CO;2. PMID 17683191.
- ↑ Hu, Y.; Hartmann, A.; Stoehr, C.; Zhang, S.; Wang, M.; Tacha, D.; Montironi, R.; Lopez-Beltran, A. et al. (Mar 2012). "PAX8 is expressed in the majority of renal epithelial neoplasms: an immunohistochemical study of 223 cases using a mouse monoclonal antibody.". J Clin Pathol 65 (3): 254-6. doi:10.1136/jclinpath-2011-200508. PMID 22135028.
- ↑ Krüger, S.; Sotlar, K.; Kausch, I.; Horny, HP. (2005). "Expression of KIT (CD117) in renal cell carcinoma and renal oncocytoma.". Oncology 68 (2-3): 269-75. doi:10.1159/000086783. PMID 16015044.
- ↑ Jain, S.; Roy, S.; Amin, M.; Acquafondata, M.; Yin, M.; Laframboise, W.; Bastacky, S.; Pantanowitz, L. et al. (Dec 2013). "Amylase α-1A (AMY1A): A Novel Immunohistochemical Marker to Differentiate Chromophobe Renal Cell Carcinoma From Benign Oncocytoma.". Am J Surg Pathol 37 (12): 1824-30. doi:10.1097/PAS.0000000000000108. PMID 24225843.
- ↑ Memeo L, Jhang J, Assaad AM, et al. (February 2007). "Immunohistochemical analysis for cytokeratin 7, KIT, and PAX2: value in the differential diagnosis of chromophobe cell carcinoma". Am. J. Clin. Pathol. 127 (2): 225–9. doi:10.1309/9KWEA4W9Y94D1AEE. PMID 17210525. http://ajcp.ascpjournals.org/cgi/pmidlookup?view=long&pmid=17210525.