Difference between revisions of "Non-malignant skin disease"
(→Solar elastosis: more) |
(rm broken) |
||
| (33 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
'''Non-malignant skin disease''' is relatively common. The pathology may or may not be specific. Some diseases require clinical information to diagnose. | '''Non-malignant skin disease''' is relatively common. The pathology may or may not be specific. Some diseases require clinical information to diagnose. | ||
An introduction to dermatopathology is in the ''[[dermatopathology]]'' article. [[Nevi]] (moles) and other melanocytic lesions are dealt with in the article ''[[melanocytic lesions]]''. Inflammatory skin conditions are dealt with in ''[[inflammatory skin disorders]]''. | An introduction to dermatopathology is in the ''[[dermatopathology]]'' article. [[Nevi]] (moles) and other melanocytic lesions are dealt with in the article ''[[melanocytic lesions]]''. Inflammatory skin conditions are dealt with in ''[[inflammatory skin disorders]]''. | ||
| Line 50: | Line 50: | ||
*[[Exocytosis]] - blood cell infiltrate the epidermis. | *[[Exocytosis]] - blood cell infiltrate the epidermis. | ||
Images | ====Images==== | ||
<gallery> | |||
Image:Dermatomycosis_-_intermed_mag.jpg | Dermatomycosis - intermed. mag. (WC) | |||
Image:Dermatomycosis_-_high_mag.jpg | Dermatomycosis - high mag. (WC) | |||
Image:Dermatomycosis_-_gms_-_low_mag.jpg | Dermatomycosis - GMS stain - low mag. (WC) | |||
Image:Dermatomycosis_-_gms_-_high_mag.jpg | Dermatomycosis - GMS stain - high mag. (WC) | |||
</gallery> | |||
www: | |||
*[http://missinglink.ucsf.edu/lm/DermatologyGlossary/img/Dermatology%20Glossary/Glossary%20Histo%20Images/tinea_pas.jpg Dermatophytosis (ucsf.edu)].<ref>URL: [http://missinglink.ucsf.edu/lm/DermatologyGlossary/tinea.html http://missinglink.ucsf.edu/lm/DermatologyGlossary/tinea.html]. Accessed on: 25 February 2013.</ref> | |||
===Stains=== | ===Stains=== | ||
| Line 79: | Line 80: | ||
==Fibroepithelial polyp== | ==Fibroepithelial polyp== | ||
{{Main|Fibroepithelial polyp}} | |||
==Actinic keratosis== | ==Actinic keratosis== | ||
| Line 270: | Line 225: | ||
=Very common - viral= | =Very common - viral= | ||
==Verruca vulgaris== | ==Verruca vulgaris== | ||
{{Main|Verruca vulgaris}} | |||
==Verruca plana== | ==Verruca plana== | ||
| Line 346: | Line 241: | ||
Notes: | Notes: | ||
*It differs from verruca vulgaris... (1) orthokeratosis, (2) flat surface and base. | *It differs from [[verruca vulgaris]]... (1) orthokeratosis, (2) flat surface and base. | ||
=Less common= | =Less common= | ||
| Line 387: | Line 282: | ||
==Clear cell acanthoma== | ==Clear cell acanthoma== | ||
{{Main|Clear cell acanthoma}} | |||
==Chondrodermatitis nodularis chronica helicis== | ==Chondrodermatitis nodularis chronica helicis== | ||
*[[AKA]] ''chondrodermatitis nodularis helicis''. | *[[AKA]] ''chondrodermatitis nodularis helicis''. | ||
*Abbreviated ''CNCH''. | *Abbreviated ''CNCH''. | ||
*[[AKA]] ''Winkler disease''.<ref>URL: [http://www.head-face-med.com/content/4/1/2 http://www.head-face-med.com/content/4/1/2]. Accessed on: 16 January 2014.</ref> | |||
* | {{Main|Chondrodermatitis nodularis chronica helicis}} | ||
==Cutaneous calcinosis== | ==Cutaneous calcinosis== | ||
*[[AKA]] ''calcinosis cutis''. | *[[AKA]] ''calcinosis cutis''. | ||
{{Main|Cutaneous calcinosis}} | |||
==Dilated pore of Winer== | ==Dilated pore of Winer== | ||
===General=== | ===General=== | ||
*Benign. | *Benign. | ||
*Looks like zit. | *Looks like a zit. | ||
===Microscopic=== | ===Microscopic=== | ||
| Line 515: | Line 304: | ||
*[[Acanthosis]]. | *[[Acanthosis]]. | ||
*Budding of epidermis (into dermis). | *Budding of epidermis (into dermis). | ||
DDx: | DDx: | ||
*[[ | *[[Pilar sheath acanthoma]]. | ||
Image: | |||
*[http:// | *[http://dermpathexpert.com/id90.html Dilated pore of Winer (dermpathexpert.com)]. | ||
=== | ==Lichenoid keratosis== | ||
*[[AKA]] ''lichen planus-like keratosis''. | |||
{{Main|Lichenoid keratosis}} | |||
- | |||
==Granuloma annulare== | ==Granuloma annulare== | ||
| Line 555: | Line 319: | ||
==Necrobiosis lipoidica== | ==Necrobiosis lipoidica== | ||
{{Main|Necrobiosis lipoidica}} | |||
==Keloid== | ==Keloid== | ||
| Line 595: | Line 327: | ||
:See also: ''[[nasopharyngeal angiofibroma]]''. | :See also: ''[[nasopharyngeal angiofibroma]]''. | ||
:Should '''not''' be confused with ''[[angiokeratoma]]''. | :Should '''not''' be confused with ''[[angiokeratoma]]''. | ||
{{Main|Angiofibroma}} | |||
==Benign fibrous papule== | ==Benign fibrous papule== | ||
| Line 639: | Line 353: | ||
Note: | Note: | ||
*Several variants exist.<ref name=pmid18032900>{{Cite journal | last1 = Jacyk | first1 = WK. | last2 = Rütten | first2 = A. | last3 = Requena | first3 = L. | title = Fibrous papule of the face with granular cells. | journal = Dermatology | volume = 216 | issue = 1 | pages = 56-9 | month = | year = 2008 | doi = 10.1159/000109359 | PMID = 18032900 }}</ref> | *Several variants exist.<ref name=pmid18032900>{{Cite journal | last1 = Jacyk | first1 = WK. | last2 = Rütten | first2 = A. | last3 = Requena | first3 = L. | title = Fibrous papule of the face with granular cells. | journal = Dermatology | volume = 216 | issue = 1 | pages = 56-9 | month = | year = 2008 | doi = 10.1159/000109359 | PMID = 18032900 }}</ref> | ||
===Images=== | |||
*[http://www.dermaamin.com/site/histopathology-of-the-skin/58-f/1739-fibrous-papule-angiofibroma-.html Fibrous papule (dermaamin.com)]. | |||
===Sign out=== | ===Sign out=== | ||
| Line 647: | Line 364: | ||
==Molluscum contagiosum== | ==Molluscum contagiosum== | ||
{{Main|Molluscum contagiosum}} | |||
==Superficial dermal infiltrates== | ==Superficial dermal infiltrates== | ||
| Line 731: | Line 397: | ||
==Mastocytosis== | ==Mastocytosis== | ||
{{Main|Mastocytosis}} | |||
==Ichthyosis== | ==Ichthyosis== | ||
| Line 789: | Line 415: | ||
==Palmar fibromatosis== | ==Palmar fibromatosis== | ||
*[[AKA]] ''Dupuytren's contracture''. | *[[AKA]] ''Dupuytren's contracture''. | ||
*[[AKA]] ''Dupuytren disease''. | *[[AKA]] ''Dupuytren disease''. | ||
{{Main|Palmar fibromatosis}} | |||
==Angiomyoma== | ==Angiomyoma== | ||
| Line 896: | Line 436: | ||
==Angiokeratoma== | ==Angiokeratoma== | ||
{{Main|Angiokeratoma}} | |||
==Inverted follicular keratosis== | ==Inverted follicular keratosis== | ||
| Line 1,006: | Line 503: | ||
:'''''Not''' to be confused with [[nodular fasciitis]]''. | :'''''Not''' to be confused with [[nodular fasciitis]]''. | ||
*[[AKA]] ''flesh-eating disease''. | *[[AKA]] ''flesh-eating disease''. | ||
{{Main|Necrotizing fasciitis}} | |||
==Porokeratosis== | ==Porokeratosis== | ||
{{Main|Porokeratosis}} | |||
==Nevus sebaceous== | ==Nevus sebaceous== | ||
*[[AKA]] ''nevus sebaceous of Jadassohn''. | *[[AKA]] ''nevus sebaceous of Jadassohn''. | ||
{{Main|Nevus sebaceous}} | |||
==Nevus lipomatosus superficialis== | ==Nevus lipomatosus superficialis== | ||
| Line 1,083: | Line 516: | ||
*[[AKA]] ''nevus lipomatosus cutaneous superficialis'', abbreviated ''NLCS''. | *[[AKA]] ''nevus lipomatosus cutaneous superficialis'', abbreviated ''NLCS''. | ||
*[[AKA]] ''nevus lipomatosus''.<ref name=pmid15677959>{{Cite journal | last1 = Kaw | first1 = P. | last2 = Carlson | first2 = A. | last3 = Meyer | first3 = DR. | title = Nevus lipomatosus (pedunculated lipofibroma) of the eyelid. | journal = Ophthal Plast Reconstr Surg | volume = 21 | issue = 1 | pages = 74-6 | month = Jan | year = 2005 | doi = | PMID = 15677959 }}</ref> | *[[AKA]] ''nevus lipomatosus''.<ref name=pmid15677959>{{Cite journal | last1 = Kaw | first1 = P. | last2 = Carlson | first2 = A. | last3 = Meyer | first3 = DR. | title = Nevus lipomatosus (pedunculated lipofibroma) of the eyelid. | journal = Ophthal Plast Reconstr Surg | volume = 21 | issue = 1 | pages = 74-6 | month = Jan | year = 2005 | doi = | PMID = 15677959 }}</ref> | ||
{{Main|Nevus lipomatosus superficialis}} | |||
=Bullous disease= | =Bullous disease= | ||
Latest revision as of 17:59, 23 April 2024
Non-malignant skin disease is relatively common. The pathology may or may not be specific. Some diseases require clinical information to diagnose.
An introduction to dermatopathology is in the dermatopathology article. Nevi (moles) and other melanocytic lesions are dealt with in the article melanocytic lesions. Inflammatory skin conditions are dealt with in inflammatory skin disorders.
Other
Lichen simplex chronicus
Prurigo nodularis
General
- Can be thought of as a localized/focal version of lichen simplex chronicus (LSC).
Gross
- Dome-shaped/raised - papular (<1 cm) or nodular (>1 cm).[2]
Microscopic
DDx:
- Lichen simplex chronicus - a more diffuse process, not a raised lesion.
Sign out
SKIN LESION, LEFT CHIN, BIOPSY: - PRURIGO NODULARIS.
Micro
The sections show a raised lesion with compact hyperkeratosis and irregular acanthosis. Spongiosis is seen focally. There is minimal hypergranulosis.
There is no thinning of the suprapapillary plate and no dilated superficial blood vessels. There is no interface activity.
Very common
Dermatomycosis
- Dermatophytosis redirects here.
General
- Fungal infection of skin.
Note:
- Dermatophytosis (ring worm) is a type of dermatomycosis.
Microscopic
Features:
- Microorganisms - key feature.
- Often hyphae (candida) - like twigs of a tree... branching.
- May be very fragmented in section ~ size of a neutrophil.
- Often hyphae (candida) - like twigs of a tree... branching.
- Perivascular inflammation, esp. neutrophils.
- Exocytosis - blood cell infiltrate the epidermis.
Images

Dermatomycosis - intermed. mag. (WC)

Dermatomycosis - high mag. (WC)

Dermatomycosis - GMS stain - low mag. (WC)
Dermatomycosis - GMS stain - high mag. (WC)




www:
Stains
Sign out
SKIN, BIOPSY: - SKIN WITH SUPERFICIAL FUNGAL ORGANISMS CONSISTENT WITH CANDIDA. - REACTIVE CHANGES OF THE EPITHELIUM.
Micro
The sections show skin with a neutrophilic infiltrate in the superficial epidermis. PAS-D staining demonstrates fungal organisms with a morphology suggestive of candida.
The epithelium has parakeratosis, acanthosis and spongiosis. No mitotic activity is appreciated. The keratinocytes are moderately enlarged and have evident nucleoli.
Cicatrix
Fibroepithelial polyp
Actinic keratosis
Actinic cheilitis
General
- Actinic keratosis of the lip.[4]
Microscopic
- See actinic keratosis.
Sign out
LESION, LOWER LIP, BIOPSY: - ACTINIC CHEILITIS. - SOLAR ELASTOSIS.
Micro
The sections show skin with moderate basal nuclear hyperchromasia and atypia, and parakeratosis. The squamous epithelium has maturation to the surface. There is no inflammation at the dermal-epidermal interface. Solar elastosis is present.
Seborrheic keratosis
Pilomatricoma
Dermatofibroma
Ezcema
General
- A nebulous thingy.
- Very common.
DDx:
- Contact allergy.
- Drug reaction.
- Food allergy.
Microscopic
Features:[5]
- Spongiosis (epidermal edema); keratinocytes spacing increased - key feature.
- +/-Interdermal vesicles.
- +/-Eosinophils (may suggest Rx reaction).
- Perivascular lymphocytes.
Acne vulgaris
General
- Extremely common - esp. among adolescents.
- Very rarely seen by pathologists.
Treatments:
- Antibiotic (minocycline).
- Isotretinoin AKA all-trans retinoic acid (ATRA).
Gross
- Papules, pustules, nodules or cysts.
- White, black or erythematous.
Images:
Microscopic
Features:[6]
- Folliculitis:[7]
- Neutrophils around hair follicle and infiltrate into it - including the follicular canal.
- Epidermal invagination or cyst at site of a hair follicle - contains:
- Sebum.
- +/-Bacteria (Propionibacterium acnes) and inflammatory cells - typically neurophils.
Subtyped into:
- Open comedones ("blackheads") - no extension to epidermal surface.
- Closed comedones ("whiteheads") - to epidermal surface have wide opening.
DDx - acneiform disorder:[7]
- Rosacea.
- Infective folliculitis.
- Perioral dermatitis.
- Acne vulgaris.
Image:
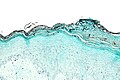
Solar elastosis
General
- Very common.
- Caused by sun exposure - specifically UV light.[9]
- Severity correlated with cumulative exposure to UV light..[10]
- Often co-localized with skin cancers - as UV light is risk factor for skin cancers.[10]
- Benign.
Microscopic
Features:
- Grey, spaghetti-like material in the superficial dermis.
DDx:
Note:
- The DDx above is things associated with sun damaged skin.
- Dermal mucin (as my be seen in lupus erythematosus) is a possible mimic - but it isn't spaghetti-like and the "background" (an interface dermatitis) is different.
Images

Solar elastosis - intermed. mag. (WC)
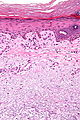
Solar elastosis - high mag. (WC)


{kind=link}
{kind=link}
www:
Sign out
SKIN, RIGHT CHEEK, RE-EXCISION: - DERMAL SCAR. - EXTENSIVE SOLAR ELASTOSIS.
Prominent blood vessels
SKIN LESION, LEFT CHEEK, BIOPSY: - SKIN WITH SOLAR ELASTOSIS AND PROMINENT SMALL BLOOD VESSELS.
SUPERIOR SHOULDER, LEFT, PUNCH BIOPSY: - BENIGN SKIN WITH MODERATE SOLAR ELASTOSIS, PROMINENT SMALL BLOOD VESSELS AND SCATTERED PERIVASCULAR LYMPHOCYTES AND PLASMA CELLS. - NEGATIVE FOR BASAL CELL CARCINOMA. - NEGATIVE FOR ACTINIC KERATOSIS.
Micro
The sections show hair bearing skin with solar elastosis and numerous small dilated blood vessels. The dermis is mildly fibrotic. Compact keratin is present.
The epidermis matures to the surface. A granular layer is present. There is no basal epidermal atypia. No melanocytic nests are identified. There is no palisading of the basal cells. Rare scattered lymphocytes are in the dermis.
Very common - viral
Verruca vulgaris
Verruca plana
General
- Common.
- Usu. hands and face.[11]
Microscopic
Features:[11]
- Orthokeratosis with basketweave pattern.
- Hypergranulosis.
- Viral keratohyaline.
- Koilocytes.
- Acanthosis - yet flat surface and base.
Notes:
- It differs from verruca vulgaris... (1) orthokeratosis, (2) flat surface and base.
Less common
Chronic folliculitis
- Folliculitis redirect here.
General
- Common.
- Infrequently biopsied.
Gross
- Erythema.[12]
DDx gross:
Microscopic
Features:
- Inflammation around the hair follicle - key feature.
- Lymphocytes - usu. predominant.
- +/-Chronic changes:
- Acanthosis.
- Hyperkeratosis.
- Hypergranulosis.
DDx:
Sign out
SKIN LESION, UPPER ARM, BIOPSY: - CHRONIC FOLLICULITIS WITH SECONDARY SURFACE CHANGES.
Micro
The sections show hair-bearing skin with abundant lymphocytes around and within the hair follicle wall.
The non-hair follicle epidermis has acanthosis, hypergranulosis and compact hyperkeratosis. There is no inflammatory cell infiltrate in the non-hair follicle epidermis or at the non-hair follicle interface.
There are no granulomas.
Clear cell acanthoma
Chondrodermatitis nodularis chronica helicis
Cutaneous calcinosis
- AKA calcinosis cutis.
Dilated pore of Winer
General
- Benign.
- Looks like a zit.
Microscopic
Features:[14]
- Dilated hair follicle with keratin.
- Acanthosis.
- Budding of epidermis (into dermis).
DDx:
Image:
Lichenoid keratosis
- AKA lichen planus-like keratosis.
Granuloma annulare
Necrobiosis lipoidica
Keloid
Angiofibroma
- See also: nasopharyngeal angiofibroma.
- Should not be confused with angiokeratoma.
Benign fibrous papule
- AKA fibrous papule.
General
- An angiofibroma on the face that is solitary.[15][16]
Gross
Microscopic
Features:[17]
- Dome-shaped.
- Fibrotic dermis.
- Enlarged fibroblasts.
- Dilated small vessels.
- +/-Multinucleated stromal cells.[18]
- +/-Stellate cells.[18]
DDx:
- Angiofibroma - not solitary or not on the nose.
Note:
- Several variants exist.[16]
Images
Sign out
SKIN LESION, CHIN, BIOPSY: - BENIGN FIBROUS PAPULE.
Molluscum contagiosum
Superficial dermal infiltrates
Discussed in detail by Alsaad and Ghazarian.[19]
Dermal perivascular lymphoeosinophilic infiltration
- Abbreviated DPLI.
Microscopic appearance is just what it is called:
- Lymphocytes and eosinophils around the vessels in the superficial dermis.
DDx:[19]
- Insect bite - classically wedge-shaped.[20]
- Drug reaction.
- Urticarial reaction.
- Prevesicular early stage of bullous pemphigoid.
- HIV related dermatoses.
Notes:
- May superficially resemble cutaneous lymphoma.[20]
Images:
{kind=link}
{kind=link}
Congenital dermal melanocytosis
- AKA Mongolian spots.
- Classically seen in asian children.
Gross:
- Brown or blue-grey patch in the lumbosacral area.
Mastocytosis
Ichthyosis
General
- Comes in different flavours.
- Usu. inherited... thus a pediatric condition.
Gross
- Fish scale-like appearance.
Image:
{kind=link}
Microscopic
Features:[21]
- Thick stratum corneum without basket-weave pattern.
Palmar fibromatosis
Angiomyoma
- Do not confuse with angiomyxoma.
General
- Benign.
- Female > male.[22]
Microscopic
Features:
- Well-circumscribed lesion with fascicular architecture.
- Spindle cells/epithelioid cell with moderate eosinophilic (pink) cytoplasm.
- Thick-walled blood vessels. (???)
Images:
{kind=link}
{kind=link}
Angiokeratoma
Inverted follicular keratosis
- Abbreviated IFK.[23]
General
- Benign skin lesion.
- Central face - middle age.[24]
- Uncommon.
- May be considered a variant of seborrheic keratosis that is predominantly endophytic.[25]
Microscopic
Features:[24]
- Keratinocyte of cytologically benign proliferation.
- "Squamous eddies" (whorls of keratin).
- Coarse keratohyaline granules.
DDx:
- Squamous cell carcinoma of the skin.
- Trichilemmoma.
- Seborrheic keratosis - has an exophytic component.
Images:
- Inverted follicular keratosis - low mag. (flickr.com).
- Inverted follicular keratosis - high mag. (flickr.com).
- Inverted follicular keratosis - several images (mckeedermpath.com).
Sign out
SKIN LESION, FACE, BIOPSY: - INVERTED FOLLICULAR KERATOSIS.
Micro
The sections show skin with acanthosis, pseudohorn cysts, and focal basal epidermal pigmentation. There is no basal nuclear atypia, no mitoses and there are no melanocytic nests. There is minimal dermal inflammation. There is no apparent solar elastosis.
Focal cutaneous mucinosis
General
- Benign.
- May be associated with systemic disease.[27]
Microscopic
Features:
- Light blue whispy material in the dermis - key feature.
DDx:
- Dermal edema.
- Digital mucous cyst.
Panniculitis
This is dealt with in the panniculitis article.
DDx for panniculitis:
- Erythema nodosum.
- Erythema induratum.
- Self-inflicted trauma.
- Systemic lupus erythematosus.
- Weird stuff.
Rare
Necrotizing fasciitis
- Not to be confused with nodular fasciitis.
- AKA flesh-eating disease.
Porokeratosis
Nevus sebaceous
- AKA nevus sebaceous of Jadassohn.
Nevus lipomatosus superficialis
- Abbreviated NLS.
- AKA nevus lipomatosus cutaneous superficialis, abbreviated NLCS.
- AKA nevus lipomatosus.[28]
Bullous disease
Cysts
See also
References
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 26. ISBN 978-0443066542.
- ↑ URL: http://www.pediatrics.wisc.edu/education/derm/text.html. Accessed on: 23 August 2012.
- ↑ URL: http://missinglink.ucsf.edu/lm/DermatologyGlossary/tinea.html. Accessed on: 25 February 2013.
- ↑ Picascia, DD.; Robinson, JK. (Aug 1987). "Actinic cheilitis: a review of the etiology, differential diagnosis, and treatment.". J Am Acad Dermatol 17 (2 Pt 1): 255-64. PMID 3305604.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1188. ISBN 978-1416031215.
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 76. ISBN 978-0443066542.
- ↑ 7.0 7.1 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 77. ISBN 978-0443066542.
- ↑ URL: http://www.dermnetnz.org/dermal-infiltrative/solar-elastosis.html. Accessed on: 27 March 2013.
- ↑ Thomas, NE.; Kricker, A.; From, L.; Busam, K.; Millikan, RC.; Ritchey, ME.; Armstrong, BK.; Lee-Taylor, J. et al. (Nov 2010). "Associations of cumulative sun exposure and phenotypic characteristics with histologic solar elastosis.". Cancer Epidemiol Biomarkers Prev 19 (11): 2932-41. doi:10.1158/1055-9965.EPI-10-0686. PMID 20802019.
- ↑ 10.0 10.1 Karagas, MR.; Zens, MS.; Nelson, HH.; Mabuchi, K.; Perry, AE.; Stukel, TA.; Mott, LA.; Andrew, AS. et al. (Mar 2007). "Measures of cumulative exposure from a standardized sun exposure history questionnaire: a comparison with histologic assessment of solar skin damage.". Am J Epidemiol 165 (6): 719-26. doi:10.1093/aje/kwk055. PMID 17204514.
- ↑ 11.0 11.1 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 480. ISBN 978-0781765275.
- ↑ URL: http://www.webmd.com/skin-problems-and-treatments/tc/folliculitis-topic-overview. Accessed on: 7 November 2012.
- ↑ URL: http://www.head-face-med.com/content/4/1/2. Accessed on: 16 January 2014.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 486. ISBN 978-0781765275.
- ↑ 15.0 15.1 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 505. ISBN 978-0443066542.
- ↑ 16.0 16.1 16.2 Jacyk, WK.; Rütten, A.; Requena, L. (2008). "Fibrous papule of the face with granular cells.". Dermatology 216 (1): 56-9. doi:10.1159/000109359. PMID 18032900.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 492. ISBN 978-0781765275.
- ↑ 18.0 18.1 Ragaz, A.; Berezowsky, V. (1979). "Fibrous papule of the face. A study of five cases by electron microscopy.". Am J Dermatopathol 1 (4): 353-6. PMID 543528.
- ↑ 19.0 19.1 Alsaad, KO.; Ghazarian, D. (Dec 2005). "My approach to superficial inflammatory dermatoses.". J Clin Pathol 58 (12): 1233-41. doi:10.1136/jcp.2005.027151. PMID 16311340.
- ↑ 20.0 20.1 Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 1269. ISBN 0-7216-0187-1.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1185. ISBN 978-1416031215.
- ↑ Katenkamp D, Kosmehl H, Langbein L (1988). "[Angiomyoma. A pathologo-anatomic analysis of 229 cases]" (in German). Zentralbl Allg Pathol 134 (4-5): 423–33. PMID 3201831.
- ↑ Shih, CC.; Yu, HS.; Tung, YC.; Tsai, KB.; Cheng, ST. (Jan 2001). "Inverted follicular keratosis.". Kaohsiung J Med Sci 17 (1): 50-4. PMID 11411260.
- ↑ 24.0 24.1 24.2 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 387. ISBN 978-0443066542.
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 341. ISBN 978-0443066542.
- ↑ URL: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC475744/. Accessed on: 11 May 2010.
- ↑ Gandhi, V.; Dogra, D.; Pandhi, RK.. "Cutaneous focal mucinosis.". Indian J Dermatol Venereol Leprol 62 (4): 260-1. PMID 20948074.
- ↑ Kaw, P.; Carlson, A.; Meyer, DR. (Jan 2005). "Nevus lipomatosus (pedunculated lipofibroma) of the eyelid.". Ophthal Plast Reconstr Surg 21 (1): 74-6. PMID 15677959.