Difference between revisions of "Panniculitis"
Jump to navigation
Jump to search
m (→DDx by type) |
|||
| Line 59: | Line 59: | ||
*[http://missinglink.ucsf.edu/lm/DermatologyGlossary/img/Dermatology%20Glossary/Glossary%20Histo%20Images/Erythema_Nodosum_high_power.jpg EN - high mag. (ucsf.edu)]. | *[http://missinglink.ucsf.edu/lm/DermatologyGlossary/img/Dermatology%20Glossary/Glossary%20Histo%20Images/Erythema_Nodosum_high_power.jpg EN - high mag. (ucsf.edu)]. | ||
== | ==Morphea profunda== | ||
*[[AKA]] '' | *[[AKA]] ''scleroderma panniculitis''. | ||
===General=== | ===General=== | ||
Revision as of 19:46, 19 September 2011
Panniculitis is inflammation of the adipose tissue. It is encountered in dermatopathology specimens.
Classification
- Lobular - involve fat lobules.
- Septal - involve interlobular septae.
A simple general DDx
- Erythema nodosum.
- Erythema induratum.
- Self-inflicted trauma (factitial panniculitis).
- Systemic lupus erythematosus.
- Other.
DDx by type
Septal:
- Erythema nodosum.
- Scleroderma panniculitis, also morphea profunda.[1]
Lobular:[1]
- Infectious panniculitis.
- Erythema induratum.
- Lupus panniculitis.
- Pancreatic panniculitis.
- Alpha1-antitrypsin deficiency.
- Subcutaneous fat necrosis of the newborn.
- Sclerema neonatorum.
Specific conditions
Erythema nodosum
Causes - mnemonic NODOSUM:[2]
- NO cause (idiopathic) ~ 55% of cases.
- Drugs (sulfonamides, amoxicillin, oral contraceptives) ~ 5% of cases.
- Other infections - group A streptococci (streptococcal pharyngitis), Yersinia, chlamydia, mycobacteria, others ~ 30% of cases.
- Sarcoidosis ~ 7% of cases.
- Ulcerative colitis & Crohn's disease ~ 2% of cases.
- Malignancy (leukemia, Hodgkin's lymphoma) ~ 1% of cases
Microscopic
- Expanded septa between fat lobules - key (low power) feature.
- Neutrophils.
- Lymphocytes.
- Histiocytes.
- Fibrin.
Notes:
- No vasculitis.
- +/-Granulomas.[6]
DDx:
Images:
{kind=link}
{kind=link}
Morphea profunda
- AKA scleroderma panniculitis.
General
Main article: Scleroderma
- Think about the name... sclerotic (sclero-) dermis (-derma).
Microscopic
Features:[1]
- Septal fibrosis/expansion - key feature.
- Classically ~2-3x an adiposcyte thick.
- +/-Deep dermal perivascular lymphocytes and plasma cells.
DDx:
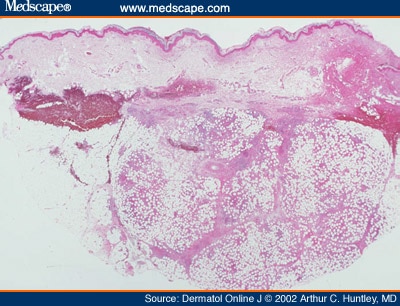
Erythema induratum
General
Features:[4]
- Uncommon.
- Etiology: unknown.
Clinical:[5]
- Classic location: posterior shins.
- Ulcerates and scars.
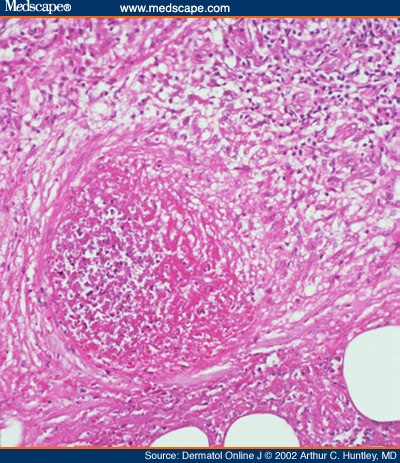
Microscopic
Features:[4]
- Predominantly lobular process with:[3]
- Necrotizing granulomatous inflammation.
- Necrotizing vasculitis of small/medium sized vessels (early).
DDx:
- Infection.
Images:
{kind=link}
{kind=link}
See also
References
- ↑ 1.0 1.1 1.2 Brinster, NK. (Nov 2008). "Dermatopathology for the surgical pathologist: a pattern-based approach to the diagnosis of inflammatory skin disorders (part II).". Adv Anat Pathol 15 (6): 350-69. doi:10.1097/PAP.0b013e31818b1ac6. PMID 18948765.
- ↑ 2.0 2.1 Schwartz, RA.; Nervi, SJ. (Mar 2007). "Erythema nodosum: a sign of systemic disease.". Am Fam Physician 75 (5): 695-700. PMID 17375516.
- ↑ 3.0 3.1 URL: http://www.medscape.com/viewarticle/440356_8. Accessed on: 11 September 2011.
- ↑ 4.0 4.1 4.2 Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1199. ISBN 978-1416031215.
- ↑ 5.0 5.1 Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 609. ISBN 978-1416054542.
- ↑ 6.0 6.1 URL: http://missinglink.ucsf.edu/lm/DermatologyGlossary/erythema_nodosum.html. Accessed on: 11 September 2011.