Difference between revisions of "Diffuse astrocytoma"
Jump to navigation
Jump to search
Jensflorian (talk | contribs) (not complete) |
Jensflorian (talk | contribs) (+pic) |
||
| Line 22: | Line 22: | ||
*No necrosis, no vascular proliferations. | *No necrosis, no vascular proliferations. | ||
==IHC== | |||
*[[GFAP]]+ve. | *[[GFAP]]+ve. | ||
*[[MAP2]]+ve (especially in cell processes). | *[[MAP2]]+ve (especially in cell processes). | ||
| Line 31: | Line 31: | ||
*[[ATRX]] loss in 70%. | *[[ATRX]] loss in 70%. | ||
==Molecular== | |||
*Absence of LOH 1p/19q. | *Absence of LOH 1p/19q. | ||
*Tp53 mutations in approx. 60% (80-90% in gemistocytic, 50% in fibrillary types). | *Tp53 mutations in approx. 60% (80-90% in gemistocytic, 50% in fibrillary types). | ||
| Line 39: | Line 39: | ||
*Reactive astrocytosis. | *Reactive astrocytosis. | ||
*Demyelinisation. | *Demyelinisation. | ||
*[[Anaplastic astrocytoma]] | |||
*[[Oligoastrocytoma]] | |||
*[[Oligodendroglioma]] - esp. protoplasmatic forms. | |||
*[[SEGA]] - esp. gemistocytic forms. | |||
<gallery> | <gallery> | ||
File:Diffuse_astrocytoma_HE_stain.jpg | DIffuse astrocytoma, [[H&E]] (WC/jensflorian) | |||
File:Astrocytoma whoII HE.jpg | Astrocytoma, fibrillary type (WC/jensflorian) | File:Astrocytoma whoII HE.jpg | Astrocytoma, fibrillary type (WC/jensflorian) | ||
File:Neuropathology case II 02.jpg | Astrocytoma, protoplasmatic type (WC/jensflorian) | File:Neuropathology case II 02.jpg | Astrocytoma, protoplasmatic type (WC/jensflorian) | ||
Revision as of 06:26, 22 October 2015
Diffuse astrocytoma (AKA: diffuse, low-grade astrocytoma) is a infiltrating astrocytoma occurring in the CNS white matter.
- Most common grade II WHO glioma in adults (peaks between 30-40 years).
- 10-15% of all astrocytomas.
- Usually shows progression to glioblastoma sooner or later.
Previously categorized as follows:The International Agency for Research on Cancer (Editors: Louis, D.N.; Ohgaki, H.; Wiestler, O.D.; Cavenee, W.K.) (2007). Pathology and Genetics of Tumours of Tumors of the Central Nervous System (IARC WHO Classification of Tumours) (4th ed.). Lyon: World Health Organization. pp. 25. doi:10.1007/s00401-007-0243-4. ISBN 978-9283224303.
- Diffuse astrocytoma ICD-O: 9400/3
- Fibrillary astrocytoma ICD-O: 9420/3 - most frequent
- Gemistocytic astrocytoma ICD-O:9411/3
- Protoplasmatic astrocytoma ICD-O:9410/3 - rare
Note: This subtyping is no longer in use!
Histology
- Cell density higher than normal brain.
- Mild to moderate nuclear pleomorphism.
- Monotony of atypical nuclei hints at neoplasm.
- Cytoplasm highly variable (even within the same tumour).
- In normal CNS the cytoplasm blends within the neuropil.
- Mitoses absent or very rare.
- Microcystic changes of the background (none to extensive).
- No necrosis, no vascular proliferations.
IHC
- GFAP+ve.
- MAP2+ve (especially in cell processes).
- Vimentin+ve (often perinuclear).
- S-100+ve.
- MIB-1: 0-5% (mean: 2%).
- IDH-1 (R132H)+ve in 60-70%.
- ATRX loss in 70%.
Molecular
- Absence of LOH 1p/19q.
- Tp53 mutations in approx. 60% (80-90% in gemistocytic, 50% in fibrillary types).
- MGMT promotor methylated in approx. 50%.
DDx
- Reactive astrocytosis.
- Demyelinisation.
- Anaplastic astrocytoma
- Oligoastrocytoma
- Oligodendroglioma - esp. protoplasmatic forms.
- SEGA - esp. gemistocytic forms.
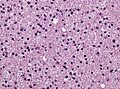
DIffuse astrocytoma, H&E (WC/jensflorian)
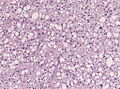
Astrocytoma, fibrillary type (WC/jensflorian)
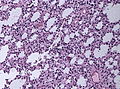
Astrocytoma, protoplasmatic type (WC/jensflorian)


