Difference between revisions of "Chronic cholecystitis"
Jump to navigation
Jump to search
| Line 78: | Line 78: | ||
==Sign out== | ==Sign out== | ||
<pre> | |||
Gallbladder, Cholecystectomy: | |||
- Cholelithiasis. | |||
- Chronic cholecystitis, mild. | |||
- One benign lymph node. | |||
</pre> | |||
====Block letters==== | |||
<pre> | <pre> | ||
GALLBLADDER, CHOLECYSTECTOMY: | GALLBLADDER, CHOLECYSTECTOMY: | ||
Revision as of 21:27, 18 August 2015
| Chronic cholecystitis | |
|---|---|
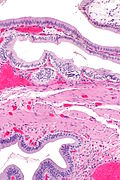
| Diagnosis in short | |
 Chronic cholecystitis with cholesterolosis. H&E stain. | |
|
| |
| LM | entrapped epithelial crypts, fibrosis/muscular hypertrophy of gallbladder wall, +/-foamy macrophages |
| LM DDx | acute cholecystitis, gallbladder adenocarcinoma, gallbladder adenomyoma, intestinal metaplasia of the gallbladder |
| Gross | +/-strawberry-like appearance, yellow stones, fibrotic wall |
| Site | gallbladder |
|
| |
| Associated Dx | cholelithiasis, gallbladder cholesterolosis, obesity |
| Clinical history | biliary colic, usu. fertile fat females forty years or less |
| Symptoms | constant right upper quadrant pain after a meal (biliary colic) |
| Prevalence | very common |
| Prognosis | good, benign |
Chronic cholecystitis, abbreviated CC, is a very common pathology of the gallbladder and increasing in prevalence with the expanding waist lines.
General
Epidemiology
- Female, fat, fertile, family history, forty (though now getting younger... as people get fatter).
Etiology
- Cholelithiasis.
- Thick bile (acalculous cholecystitis).
Clinical (classic)
- Constant right upper quadrant pain after a fatty meal (biliary colic).
- Positive Murphy's sign (physical exam, with ultrasound).
Gross
- +/-Cholelithiasis - strongly associated pathology.
- +/-Strawberry-like appearance - common (due to gallbladder cholesterolosis).
- Small ridges (microvillus architecture) + yellow.
- Normal gallbladder mucosa = smooth, green.
- Small ridges (microvillus architecture) + yellow.
- +/-Congestion/erythema.
- +/-Wall thickening - typically ~ 6-7 mm.[1]
Note:
- Wall thickening (due to congestion/edema) is the important gross finding in acute cholecystitis.
- Wall thickenss greater than 10 mm should raise the suspicion of malignancy.[1]
Microscopic
Features:[2]
- Thickening of the gallbladder wall - due to fibrosis/muscular hypertrophy - key feature.
- Chronic inflammatory cells - usu. "minimal".
- Lymphocytes - most common.
- Rokitansky-Aschoff sinuses - common.[3]
- Entrapped epithelial crypts -- pockets of epithelium in the wall of the gallbladder.
- +/-Foamy macrophages in the lamina propria (cholesterolosis of the gallbladder).
DDx:
- Gallbladder cholesterolosis and chronic cholecystitis.
- Gallbladder adenomyoma.
- Acute cholecystitis - more inflammation, lack Rokitansky-Aschoff sinuses, +/-mucosal erosions.
- Cholecystectomy for gallstone pancreatitis - intraepithelial neutrophil clusters common, history essential.
- Intestinal metaplasia of the gallbladder - goblet cells present, may be focal.
- Gallbladder adenocarcinoma.
Images
CC - intermed. mag. (WC)

Cholesterolosis. (WC)


Sign out
Gallbladder, Cholecystectomy: - Cholelithiasis. - Chronic cholecystitis, mild. - One benign lymph node.
Block letters
GALLBLADDER, CHOLECYSTECTOMY: - CHRONIC CHOLECYSTITIS. - CHOLELITHIASIS.
Without stones
GALLBLADDER, CHOLECYSTECTOMY: - CHRONIC CHOLECYSTITIS. - NO GALLSTONES IDENTIFIED.
Liver present
GALLBLADDER, CHOLECYSTECTOMY: - CHRONIC CHOLECYSTITIS. - CHOLELITHIASIS. - SMALL AMOUNT OF LIVER WITHOUT APPARENT PATHOLOGY.
GALLBLADDER, CHOLECYSTECTOMY: - CHRONIC CHOLECYSTITIS WITH MILD CHOLESTEROLOSIS. - CHOLELITHIASIS. - SMALL AMOUNT OF LIVER WITH CAUTERY/CRUSH ARTIFACT.
Micro
The sections shows gallbladder wall with Rokitansky-Aschoff sinuses and a moderate mixed inflammatory infiltrate predominantly consisting of lymphocytes. No nuclear atypia is seen.
Post-cholecystostomy tube
The sections shows gallbladder wall with edema, a moderate mixed inflammatory infiltrate (predominantly consisting of lymphocytes and plasma cells), and mucosal erosions. Reactive fibroblasts and hemosiderin-laden macrophages are present. No significant nuclear changes are seen. One benign lymph node is present.
See also
References
- ↑ 1.0 1.1 Kim, HJ.; Park, JH.; Park, DI.; Cho, YK.; Sohn, CI.; Jeon, WK.; Kim, BI.; Choi, SH. (Feb 2012). "Clinical usefulness of endoscopic ultrasonography in the differential diagnosis of gallbladder wall thickening.". Dig Dis Sci 57 (2): 508-15. doi:10.1007/s10620-011-1870-0. PMID 21879282.
- ↑ Iacobuzio-Donahue, Christine A.; Montgomery, Elizabeth A. (2005). Gastrointestinal and Liver Pathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 439. ISBN 978-0443066573.
- ↑ URL: http://www.whonamedit.com/synd.cfm/983.html. Accessed on: 29 October 2011.