Difference between revisions of "Pneumonia"
Jump to navigation
Jump to search
(more) |
|||
| Line 1: | Line 1: | ||
'''Pneumonia''' is inflammation of the lung and | '''Pneumonia''' is inflammation of the lung, which includes infectious and non-infectious etiologies. | ||
It is a subset of the [[medical lung diseases]]. This article primarily deals with the infectious pneumonias. [[Idiopathic interstitial pneumonia]]s are discussed very briefly and dealt with in detail in the ''[[diffuse lung diseases]]'' article. | |||
=Infectious pnemonia= | =Infectious pnemonia= | ||
Revision as of 23:00, 18 March 2012
Pneumonia is inflammation of the lung, which includes infectious and non-infectious etiologies.
It is a subset of the medical lung diseases. This article primarily deals with the infectious pneumonias. Idiopathic interstitial pneumonias are discussed very briefly and dealt with in detail in the diffuse lung diseases article.
Infectious pnemonia
Anatomical classification of pneumonia
- Generally, not used by clinicians.
- Use of the terms without qualification is discouraged... as they do not make explicit the etiology.
Bronchopneumonia
- Multiple foci of (acute) inflammation involving the bronchi.
- This is the most common form of (infectious) pneumonia.
Lobar pneumonia
- Pneumonia that involves a whole lobe.
- Rarely seen in areas where antibiotic treatments are widely available.
Acute infectious pneumonia
General
- This is seen by pathologists, in autopsy, from time-to-time.
Most common cause:
- Streptococcus pneumoniae.[1]
The top three community acquired (acute) pneumonia:[2]
- Streptococcuc pneumonia.
- Haemophilus influenzae.
- Moraxella catarrhalis.
Other community acquired pneumonia:[1]
- S. aureus.
- Legionaella pneumophila.
- Klebsiella pneumoniae.
- Pseudomonas.
Hospital-acquired pneumonia:[1]
- Gram-negative rods.
- Staphylococcus aureus.
Radiologic correlate
- Air space disease.
Gross pathology
- Consolidation (the lung parenchyma is firm) - best appreciated by running a finger over the cut surface of the lung with a small-to-moderate amount of pressure.
Bronchopneumonia:
- Classically yellow-white centered on the bronchi.[3]
Lobar pneumnia is classically described in four stages:[4][5]
- Congestion - day 1-2.
- Red hepatization - day 2-4.
- Gray hepatization - day 4-6.
- Resolution - day 6+.
Note:
- The stages of lobar pneumonia is considered more-or-less historical. In the age of antibiotics, lobar pneumonia is uncommon.
Microscopic
Features:
- Alveoli packed with PMNs.
- +/-Clusters of bacteria - small dots or rods.
- +/-Abscess formation.
- Lung abscess = destruction of parenchyma + PMNs.[6]
Image:
{kind=link}
Stains
- Gram stain -- to type the bacteria.
Chronic infectious pneumonia
General
Common microorganisms:[1]
- Nocardia.
- Actinomyces.
- Mycobacterium tuberculosis.
- Atypical mycobacterium, e.g. Mycobacterium avium-intracellulare.
- Histoplasma capsulatum.
- Coccidioides immitis.
- Blastomyces dermatitidis.
Note:
- All of the later ones are granulomatous.
Microscopic
Features:
- Inflammation.
- +/-Granulomas.
Aspiration pneumonia
General
- Usually seen in the context of a toxin and/or pathology that affects the swallowing and cough reflexes.[7]
- Stroke.
- Multiple sclerosis.
- Alcohol.
- The microorganisms involved are usually different than in other causes of acute pneumonia.
Gross
- More common in the right lung.
- Right main stem bronchus is more vertical.
Microscopic
Features:
- +/-Foreign body giant cells.
- Microorganisms.
Images:
{kind=link}
{kind=link}
{kind=link}
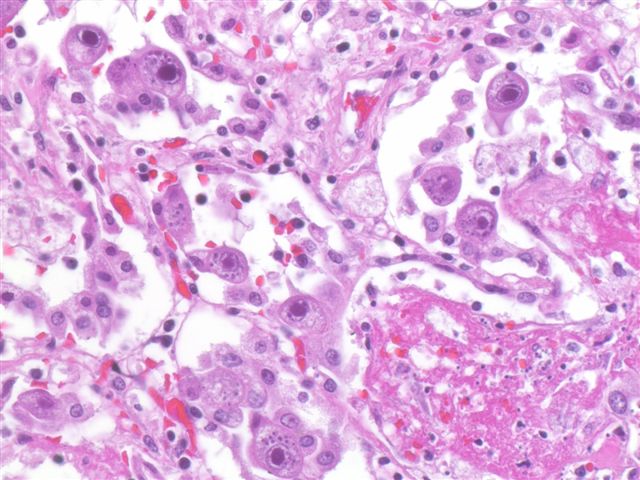
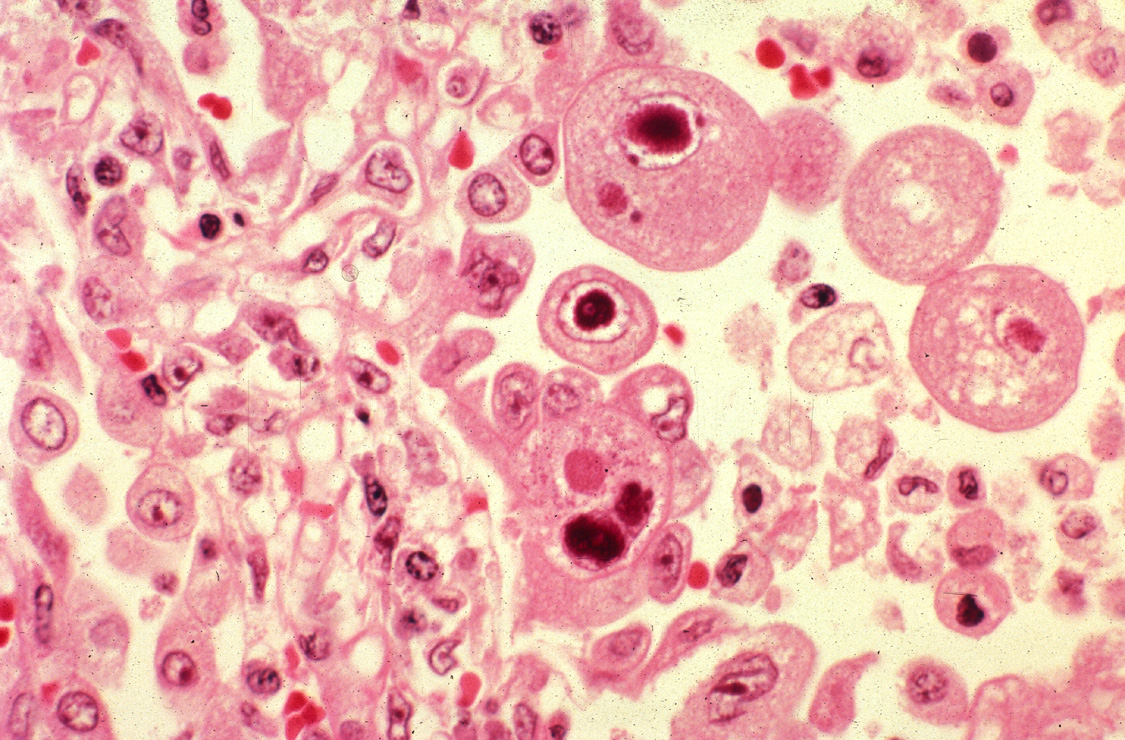
Cytomegalovirus pneumonia
Main article: Cytomegalovirus
General
- Immunodeficiency.
- Critical illness.[8]
Microscopic
Features:
- CMV nuclear changes:
- Large red nucleus with a pale halo.
- Eosinophilic granular cytoplasmic inclusions.
Images:
{kind=link}
{kind=link}
IHC
- CMV +ve -- cytoplasmic inclusions, large nucleus.
Diffuse lung diseases
Main article: Diffuse lung disease
- AKA idiopathic interstitial pneumonia.
Histologic pattern:
- Organizing pneumonia.
- Usual interstitial pneumonia.
- Nonspecific interstitial pneumonia.
- Lymphocytic interstitial pneumonia.
- Desquamative interstitial pneumonia.
- Diffuse alveolar damage.
See also
References
- ↑ 1.0 1.1 1.2 1.3 Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 711. ISBN 978-1416031215.
- ↑ Nicolau, D. (Sep 2002). "Clinical and economic implications of antimicrobial resistance for the management of community-acquired respiratory tract infections.". J Antimicrob Chemother 50 Suppl S1: 61-70. PMID 12239229.
- ↑ Rose, Alan G. (2008). Atlas of Gross Pathology with Histologic Correlation (1st ed.). Cambridge University Press. pp. 93. ISBN 978-0521868792.
- ↑ Rose, Alan G. (2008). Atlas of Gross Pathology with Histologic Correlation (1st ed.). Cambridge University Press. pp. 92. ISBN 978-0521868792.
- ↑ URL: http://www.histopathology-india.net/Lobar_Pneumonia.htm. Accessed on: 27 February 2012.
- ↑ Rose, Alan G. (2008). Atlas of Gross Pathology with Histologic Correlation (1st ed.). Cambridge University Press. pp. 95. ISBN 978-0521868792.
- ↑ Ohrui, T. (Sep 2005). "Preventive strategies for aspiration pneumonia in elderly disabled persons.". Tohoku J Exp Med 207 (1): 3-12. PMID 16082150.
- ↑ Limaye, AP.; Boeckh, M. (Nov 2010). "CMV in critically ill patients: pathogen or bystander?". Rev Med Virol 20 (6): 372-9. doi:10.1002/rmv.664. PMID 20931610.
- ↑ URL: http://www.pathologyoutlines.com/topic/lungnontumorCMV.html. Accessed on: 23 January 2012.