Difference between revisions of "Sessile serrated adenoma"
Jump to navigation
Jump to search
(+cat.) |
(split-out) |
||
| Line 1: | Line 1: | ||
{{ Infobox diagnosis | |||
| Name = {{PAGENAME}} | |||
| Image = sessile_serrated_adenoma_3_very_high_mag.jpg | |||
| Width = | |||
| Caption = SSA. [[H&E stain]]. | |||
| Micro = serrated epithelium, crypt base dilation, crypt branching, boot-shaped glands, horizontal glands | |||
| Subtypes = | |||
| LMDDx = [[hyperplastic polyp]], [[tubular adenoma]] (when with dysplasia) | |||
| Stains = | |||
| IHC = | |||
| EM = | |||
| Molecular = | |||
| IF = | |||
| Gross = | |||
| Grossing = | |||
| Site = [[colon]] - usually cecum or ascending colon | |||
| Assdx = [[colorectal adenocarcinoma]], [[hyperplastic polyp]] | |||
| Syndromes = [[serrated polyposis syndrome]] | |||
| Signs = | |||
| Symptoms = | |||
| Prevalence = common | |||
| Bloodwork = | |||
| Rads = | |||
| Endoscopy = flat, usually > 5 mm, mucinous cap | |||
| Prognosis = | |||
| Other = | |||
| ClinDDx = normal, hyperplastic polyp | |||
}} | |||
'''Sessile serrated adenoma''', abbreviated ''SSA'', is a premalignant [[GI polyps|polyp]] of the large bowel. | |||
It is also known as ''sessile serrated polyp'' (abbreviated ''SSP''), ''sessile serrated lesion'' and ''sessile serrated adenoma/polyp'' (abbreviated ''SSA/P''). | |||
==General== | |||
*Colonic lesion. | |||
*May be seen in the context of ''[[serrated polyposis syndrome]]''. | |||
Epidemiology: | |||
*Thought to lead to colorectal cancer through a different pathway that most tumours in the left colon/rectum. | |||
*''Microvesicular [[hyperplastic polyp]]s'' are hypothesized to be the the precursor of SSAs.<ref name=pmid21045813>{{Cite journal | last1 = Huang | first1 = CS. | last2 = Farraye | first2 = FA. | last3 = Yang | first3 = S. | last4 = O'Brien | first4 = MJ. | title = The clinical significance of serrated polyps. | journal = Am J Gastroenterol | volume = 106 | issue = 2 | pages = 229-40; quiz 241 | month = Feb | year = 2011 | doi = 10.1038/ajg.2010.429 | PMID = 21045813 }}</ref> | |||
==Gross== | |||
Features:<ref name=pmid22710576/> | |||
*Flat lesions, usually > 5 mm. | |||
*Typically have a "mucous cap" - present ~65% of the time; useful for identification. | |||
*Border not well-demarcated. | |||
*More common in the proximal colon. | |||
Note: | |||
*Sessile lesions over 1 cm are usually SSAs.<ref name=pmid22710576/> | |||
Image: | |||
*[http://www.nature.com/ajg/journal/v105/n12/fig_tab/ajg2010330f1.html SSA - endoscopy (nature.com)].<ref name=pmid21131934>{{cite journal |author=Rex DK, Hewett DG, Snover DC |title=Editorial: Detection targets for colonoscopy: from variable detection to validation |journal=Am. J. Gastroenterol. |volume=105 |issue=12 |pages=2665–9 |year=2010 |month=December |pmid=21131934 |doi=10.1038/ajg.2010.330 |url=}}</ref> | |||
==Microscopic== | |||
Features: | |||
*Serrated epithelium at the surface and deep in the crypts. | |||
**Saw-tooth appearance, epithelium has jagged appearing edge. | |||
*Crypt dilation at base with serrations - '''key feature'''. | |||
**Very common -- anecdotally the most sensitive feature. | |||
*"Boot"-shape or "L"-shaped glands. | |||
**Shape may be similar to a hockey stick. | |||
*Horizontal crypts = crypt long axis parallel to the muscularis mucosae. | |||
*Crypt branching. | |||
Minimal extent criteria - number of abnormal crypts with the above features: | |||
*''German Society of Pathology'' proposal: at least two abnormal crypts -- crypts do not have to be adjacent.<ref name=pmid23052370>{{Cite journal | last1 = Ensari | first1 = A. | last2 = Bilezikçi | first2 = B. | last3 = Carneiro | first3 = F. | last4 = Doğusoy | first4 = GB. | last5 = Driessen | first5 = A. | last6 = Dursun | first6 = A. | last7 = Flejou | first7 = JF. | last8 = Geboes | first8 = K. | last9 = de Hertogh | first9 = G. | title = Serrated polyps of the colon: how reproducible is their classification? | journal = Virchows Arch | volume = 461 | issue = 5 | pages = 495-504 | month = Nov | year = 2012 | doi = 10.1007/s00428-012-1319-7 | PMID = 23052370 }}</ref><ref name=pmid20617338>{{Cite journal | last1 = Aust | first1 = DE. | last2 = Baretton | first2 = GB. | title = Serrated polyps of the colon and rectum (hyperplastic polyps, sessile serrated adenomas, traditional serrated adenomas, and mixed polyps)-proposal for diagnostic criteria. | journal = Virchows Arch | volume = 457 | issue = 3 | pages = 291-7 | month = Sep | year = 2010 | doi = 10.1007/s00428-010-0945-1 | PMID = 20617338 }}</ref> | |||
**[[Onlinepathology]] prefers this definition. | |||
*An expert panel lead by ''Rex'' states that one unequivocally altered crypt should prompt calling SSA.<ref name=pmid22710576>{{Cite journal | last1 = Rex | first1 = DK. | last2 = Ahnen | first2 = DJ. | last3 = Baron | first3 = JA. | last4 = Batts | first4 = KP. | last5 = Burke | first5 = CA. | last6 = Burt | first6 = RW. | last7 = Goldblum | first7 = JR. | last8 = Guillem | first8 = JG. | last9 = Kahi | first9 = CJ. | title = Serrated lesions of the colorectum: review and recommendations from an expert panel. | journal = Am J Gastroenterol | volume = 107 | issue = 9 | pages = 1315-29; quiz 1314, 1330 | month = Sep | year = 2012 | doi = 10.1038/ajg.2012.161 | PMID = 22710576 }}</ref> | |||
*The WHO requires - depending on what you read: | |||
**Three adjacent crypts to be abnormal.<ref>URL: [http://surgpathcriteria.stanford.edu/gitumors/sessile-serrated-polyp-adenoma/ http://surgpathcriteria.stanford.edu/gitumors/sessile-serrated-polyp-adenoma/]. Accessed on: 26 September 2012.</ref> | |||
**Two or three adjacent crypts to be abnormal.<ref name=pmid23052370/> | |||
Notes: | |||
*Typically do not have nuclear atypia, i.e. no nuclear crowding, no nuclear hyperchromasia, no cigar-shaped nuclei. | |||
**SSAs with nuclear atypia may be referred to as ''advanced sessile serrated adenomas''. | |||
===DDx=== | |||
*[[Hyperplastic polyp]]. | |||
*[[Tubular adenoma of the gastrointestinal tract|Tubular adenoma]] - for ''SSA with dysplasia'', TAs often less than 1 cm (uncommon for SSAs). | |||
===Images=== | |||
<gallery> | |||
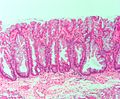
Image:Sessile_serrated_adenoma.jpg | SSA - low mag. (WC/Nephron) | |||
Image:Sessile_serrated_adenoma2.jpg | SSA - intermed. mag. (WC/Nephron) | |||
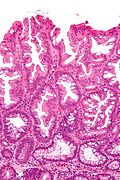
Image:Sessile_serrated_adenoma3.jpg | SSA - high mag. (WC/Nephron) | |||
Image:Sessile_serrated_adenoma_3_low_mag.jpg | SSA - low mag. (WC/Nephron) | |||
Image:Sessile_serrated_adenoma_3_intermed_mag.jpg | SSA - intermed. mag. (WC/Nephron) | |||
Image:Sessile_serrated_adenoma_3_very_high_mag.jpg | SSA - very high mag. (WC/Nephron) | |||
</gallery> | |||
==Sign out== | |||
<pre> | |||
COLONIC POLYP, ASCENDING COLON, BIOPSY: | |||
- SESSILE SERRATED ADENOMA. | |||
- NEGATIVE FOR DYSPLASIA. | |||
</pre> | |||
<pre> | |||
COLONIC POLYP, ASCENDING COLON, BIOPSY: | |||
- SESSILE SERRATED ADENOMA WITH DYSPLASIA. | |||
</pre> | |||
Note: | |||
*The above exactly mirrors the Canadian consensus.<ref name=driman>{{cite journal | last1 = Driman | first1 = DK. | last2 = Marcus | first2 = VA. | last3 = Hilsden | first3 = RJ | last4 = Owen | first4 = DA |title=Pathologic reporting of colorectal polyps: pan-Canadian consensus guidelines |journal=Canadian Journal of Pathology |volume=4 |issue=3 |pages=81-90 |year=2012 |month= |pmid= |doi= |url= }}</ref> | |||
==References== | |||
{{Reflist|2}} | |||
[[Category:Gastrointestinal pathology]] | |||
[[Category:Diagnosis]] | [[Category:Diagnosis]] | ||
Revision as of 00:51, 13 June 2013
| Sessile serrated adenoma | |
|---|---|
| Diagnosis in short | |
 SSA. H&E stain. | |
|
| |
| LM | serrated epithelium, crypt base dilation, crypt branching, boot-shaped glands, horizontal glands |
| LM DDx | hyperplastic polyp, tubular adenoma (when with dysplasia) |
| Site | colon - usually cecum or ascending colon |
|
| |
| Associated Dx | colorectal adenocarcinoma, hyperplastic polyp |
| Syndromes | serrated polyposis syndrome |
|
| |
| Prevalence | common |
| Endoscopy | flat, usually > 5 mm, mucinous cap |
| Clin. DDx | normal, hyperplastic polyp |
Sessile serrated adenoma, abbreviated SSA, is a premalignant polyp of the large bowel.
It is also known as sessile serrated polyp (abbreviated SSP), sessile serrated lesion and sessile serrated adenoma/polyp (abbreviated SSA/P).
General
- Colonic lesion.
- May be seen in the context of serrated polyposis syndrome.
Epidemiology:
- Thought to lead to colorectal cancer through a different pathway that most tumours in the left colon/rectum.
- Microvesicular hyperplastic polyps are hypothesized to be the the precursor of SSAs.[1]
Gross
Features:[2]
- Flat lesions, usually > 5 mm.
- Typically have a "mucous cap" - present ~65% of the time; useful for identification.
- Border not well-demarcated.
- More common in the proximal colon.
Note:
- Sessile lesions over 1 cm are usually SSAs.[2]
Image:
Microscopic
Features:
- Serrated epithelium at the surface and deep in the crypts.
- Saw-tooth appearance, epithelium has jagged appearing edge.
- Crypt dilation at base with serrations - key feature.
- Very common -- anecdotally the most sensitive feature.
- "Boot"-shape or "L"-shaped glands.
- Shape may be similar to a hockey stick.
- Horizontal crypts = crypt long axis parallel to the muscularis mucosae.
- Crypt branching.
Minimal extent criteria - number of abnormal crypts with the above features:
- German Society of Pathology proposal: at least two abnormal crypts -- crypts do not have to be adjacent.[4][5]
- Onlinepathology prefers this definition.
- An expert panel lead by Rex states that one unequivocally altered crypt should prompt calling SSA.[2]
- The WHO requires - depending on what you read:
Notes:
- Typically do not have nuclear atypia, i.e. no nuclear crowding, no nuclear hyperchromasia, no cigar-shaped nuclei.
- SSAs with nuclear atypia may be referred to as advanced sessile serrated adenomas.
DDx
- Hyperplastic polyp.
- Tubular adenoma - for SSA with dysplasia, TAs often less than 1 cm (uncommon for SSAs).
Images

SSA - low mag. (WC/Nephron)
SSA - intermed. mag. (WC/Nephron)

SSA - high mag. (WC/Nephron)

SSA - low mag. (WC/Nephron)
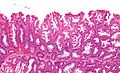
SSA - intermed. mag. (WC/Nephron)
SSA - very high mag. (WC/Nephron)





Sign out
COLONIC POLYP, ASCENDING COLON, BIOPSY: - SESSILE SERRATED ADENOMA. - NEGATIVE FOR DYSPLASIA.
COLONIC POLYP, ASCENDING COLON, BIOPSY: - SESSILE SERRATED ADENOMA WITH DYSPLASIA.
Note:
- The above exactly mirrors the Canadian consensus.[7]
References
- ↑ Huang, CS.; Farraye, FA.; Yang, S.; O'Brien, MJ. (Feb 2011). "The clinical significance of serrated polyps.". Am J Gastroenterol 106 (2): 229-40; quiz 241. doi:10.1038/ajg.2010.429. PMID 21045813.
- ↑ 2.0 2.1 2.2 Rex, DK.; Ahnen, DJ.; Baron, JA.; Batts, KP.; Burke, CA.; Burt, RW.; Goldblum, JR.; Guillem, JG. et al. (Sep 2012). "Serrated lesions of the colorectum: review and recommendations from an expert panel.". Am J Gastroenterol 107 (9): 1315-29; quiz 1314, 1330. doi:10.1038/ajg.2012.161. PMID 22710576.
- ↑ Rex DK, Hewett DG, Snover DC (December 2010). "Editorial: Detection targets for colonoscopy: from variable detection to validation". Am. J. Gastroenterol. 105 (12): 2665–9. doi:10.1038/ajg.2010.330. PMID 21131934.
- ↑ 4.0 4.1 Ensari, A.; Bilezikçi, B.; Carneiro, F.; Doğusoy, GB.; Driessen, A.; Dursun, A.; Flejou, JF.; Geboes, K. et al. (Nov 2012). "Serrated polyps of the colon: how reproducible is their classification?". Virchows Arch 461 (5): 495-504. doi:10.1007/s00428-012-1319-7. PMID 23052370.
- ↑ Aust, DE.; Baretton, GB. (Sep 2010). "Serrated polyps of the colon and rectum (hyperplastic polyps, sessile serrated adenomas, traditional serrated adenomas, and mixed polyps)-proposal for diagnostic criteria.". Virchows Arch 457 (3): 291-7. doi:10.1007/s00428-010-0945-1. PMID 20617338.
- ↑ URL: http://surgpathcriteria.stanford.edu/gitumors/sessile-serrated-polyp-adenoma/. Accessed on: 26 September 2012.
- ↑ Driman, DK.; Marcus, VA.; Hilsden, RJ; Owen, DA (2012). "Pathologic reporting of colorectal polyps: pan-Canadian consensus guidelines". Canadian Journal of Pathology 4 (3): 81-90.