Difference between revisions of "Traditional serrated adenoma"
Jump to navigation
Jump to search
| Line 48: | Line 48: | ||
**Nuclear hyperchromasia, enlargement and pseudostratification. | **Nuclear hyperchromasia, enlargement and pseudostratification. | ||
*Villous-like architecture. | *Villous-like architecture. | ||
*Ectopic crypt foci (ECF) - short crypts oriented perpendicular normal crypts, do not reach muscularis mucosae. | *Ectopic crypt foci (ECF) - short crypts oriented perpendicular normal crypts, do not reach muscularis mucosae.‡ | ||
* | |||
Note: | |||
*‡ECF considered pathognomonic for TSA - but seen in other entities.<ref name=pmid27281826>{{Cite journal | last1 = Väyrynen | first1 = SA. | last2 = Väyrynen | first2 = JP. | last3 = Klintrup | first3 = K. | last4 = Mäkelä | first4 = J. | last5 = Tuomisto | first5 = A. | last6 = Mäkinen | first6 = MJ. | title = Ectopic crypt foci in conventional and serrated colorectal polyps. | journal = J Clin Pathol | volume = 69 | issue = 12 | pages = 1063-1069 | month = Dec | year = 2016 | doi = 10.1136/jclinpath-2015-203593 | PMID = 27281826 }}</ref> | |||
DDx:<ref>URL: [http://surgpathcriteria.stanford.edu/gitumors/traditional-serrated-adenoma/differential-diagnosis.html http://surgpathcriteria.stanford.edu/gitumors/traditional-serrated-adenoma/differential-diagnosis.html]. Accessed on: 28 May 2015.</ref> | DDx:<ref>URL: [http://surgpathcriteria.stanford.edu/gitumors/traditional-serrated-adenoma/differential-diagnosis.html http://surgpathcriteria.stanford.edu/gitumors/traditional-serrated-adenoma/differential-diagnosis.html]. Accessed on: 28 May 2015.</ref> | ||
Revision as of 15:41, 5 June 2017
| Traditional serrated adenoma | |
|---|---|
| Diagnosis in short | |
| Template:Px | |
|
| |
| LM | ectopic crypt foci (ECF), serrated, eosinophilic cytoplasm, villous-like architecture, "pine cone, fernlike, stellate pit pattern" |
| Subtypes | With and without high grade dysplasia, mixed with other types of polyps |
| LM DDx | villous adenoma, hyperplastic polyp, sessile serrated adenoma |
| IHC | CK20 in the eosinophilic cells, absent in ECF; Ki67 (MIB1) stains ECF and absent in eosinophilic cells, MUC2+, MUC5CA+, MUC6-; In areas of dysplasia TP53+, nuclear B-catenin+; p16+ in late dysplasia |
| Molecular | BRAF & KRAS |
| Site | colon - usu. left side / gastrointestinal polyps |
|
| |
| Prevalence | very rare |
| Prognosis | benign (pre-malignant) |
| Clin. DDx | other GI polyps |
| Treatment | polypectomy, q3years surveillance colonoscopy |
Traditional serrated adenoma, abbreviated TSA, are a rare type of gastrointestinal polyp.
Before the sessile serrated adenomas were recognized, these lesions were known as serrated adenomas.[1]
General
- Very rare.
- Pre-malignant.[2]
Gross
- Polypoid mass.
- Usually in the left colon.
Microscopic
Features:[3]
- Serrated - essential.
- Eosinophilic cytoplasm - key feature.
- Nuclear atypia as in tubular adenoma.
- Nuclear hyperchromasia, enlargement and pseudostratification.
- Villous-like architecture.
- Ectopic crypt foci (ECF) - short crypts oriented perpendicular normal crypts, do not reach muscularis mucosae.‡
Note:
- ‡ECF considered pathognomonic for TSA - but seen in other entities.[4]
DDx:[5]
Images
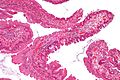
TSA - low mag. (WC/Nephron)

TSA - intermed. mag. (WC/Nephron)
- Traditional serrated adenoma very high mag.jpg
TSA - very high mag. (WC/Nephron)



TSA - low mag. (WC/Nephron)
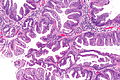
TSA - intermed. mag. (WC/Nephron)

TSA - high mag. (WC/Nephron)
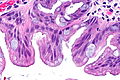
TSA - very high mag. (WC/Nephron)




{kind=link}
Sign out
Polyp, Sigmoid Colon, Polypectomy: - Traditional serrated adenoma. -- NEGATIVE for high-grade dysplasia.
Block letters
POLYP, SIGMOID COLON, POLYPECTOMY: - TRADITIONAL SERRATED ADENOMA. -- NEGATIVE FOR HIGH-GRADE DYSPLASIA.
Micro
Nonvilliform TSA
This polyp has cytologic dysplasia and serrations at the surface; however, it does not have a villiform architecture. The surface epithelium has eosinophilic cytoplasm. Overall, the morphology is most in keeping with a traditional serrated adenoma.
See also
References
- ↑ Noffsinger, AE.; Hart, J. (Jul 2010). "Serrated adenoma: a distinct form of non-polypoid colorectal neoplasia?". Gastrointest Endosc Clin N Am 20 (3): 543-63. doi:10.1016/j.giec.2010.03.012. PMID 20656251.
- ↑ Rosty, C.; Hewett, DG.; Brown, IS.; Leggett, BA.; Whitehall, VL. (Mar 2013). "Serrated polyps of the large intestine: current understanding of diagnosis, pathogenesis, and clinical management.". J Gastroenterol 48 (3): 287-302. doi:10.1007/s00535-012-0720-y. PMID 23208018.
- ↑ Li SC, Burgart L (March 2007). "Histopathology of serrated adenoma, its variants, and differentiation from conventional adenomatous and hyperplastic polyps". Arch. Pathol. Lab. Med. 131 (3): 440-5. PMID 17516746. http://journals.allenpress.com/jrnlserv/?request=get-abstract&issn=0003-9985&volume=131&page=440.
- ↑ Väyrynen, SA.; Väyrynen, JP.; Klintrup, K.; Mäkelä, J.; Tuomisto, A.; Mäkinen, MJ. (Dec 2016). "Ectopic crypt foci in conventional and serrated colorectal polyps.". J Clin Pathol 69 (12): 1063-1069. doi:10.1136/jclinpath-2015-203593. PMID 27281826.
- ↑ URL: http://surgpathcriteria.stanford.edu/gitumors/traditional-serrated-adenoma/differential-diagnosis.html. Accessed on: 28 May 2015.