Difference between revisions of "Non-invasive breast carcinoma"
(→Atypical ductal hyperplasia: split) |
|||
| Line 81: | Line 81: | ||
==Atypical ductal hyperplasia== | ==Atypical ductal hyperplasia== | ||
*Abbreviated ''ADH''. | *Abbreviated ''ADH''. | ||
{{Main|Atypical ductal hyperplasia}} | {{Main|Atypical ductal hyperplasia}} | ||
==Ductal carcinoma in situ== | ==Ductal carcinoma in situ== | ||
Revision as of 15:28, 28 April 2016
Non-invasive breast carcinoma is a type of breast cancer and a common entity... since the introduction of radiologic breast screening.
Viewed simplistically, it can neatly be divided into the discussion of two entities:
- Ductal carcinoma in situ (DCIS).
- Lobular carcinoma in situ (LCIS).
Invasive breast cancer is dealt with in the article invasive breast cancer. An introduction to the breast is found in the breast pathology article.
Ductal neoplasia
Overview
This category includes:
- Atypical ductal hyperplasia (ADH).
- Ductal carcinoma in situ (DCIS).
The difference between ADH and DCIS is:
- The degree of nuclear atypia; high grade is DCIS.
- The extent; small lesions are ADH, large lesions (low-grade) DCIS.
Is it ductal neoplasia?
FEHUT versus ADH versus DCIS
- Breast duct lumen with too many cells; this is common problem is breast pathology.[1]
- The general DDx for this scenario is: FEHUT versus ADH versus DCIS.
Notes:
- FEHUT = florid epithelial hyperplasia of the usual type, AKA epithelial hyperplasia (EH).
- ADH = atypical ductal hyperplasia.
- DCIS = ductal carcinoma in situ.
Tabular comparison - histomorphology
Comparison of FEHUT, ADH and DCIS (memory device: CLEAN = cell spacing, luminal spaces, extent/size, arch., nuclei):
| Morphology | FEHUT | ADH | DCIS |
|---|---|---|---|
| Cell spacing | varied, streaming | focal uniformity | uniform |
| Lumina | slits/irregular spaces; cells haphazardly arranged around lumen |
irregular spaces, no slits | circular "punched-out"; cells side-by-side + equally spaced @ interface |
| Extent | usually lobulocentric | limited extent | extensive |
| Architecture | irregular/swirling | DCIS-like | DCIS architecture (solid, cribriform, papillary, micropapillary) |
| Nuclei | variable, no nucleolus | hyperchromatic & uniform, usu. no nucleolus |
evenly spaced +/-nucleolus |
Treatment - implications:
- FEHUT - nothing; FEHUT is benign.
- ADH - simple excision, i.e. lumpectomy.
- DCIS - excision (lumpectomy) + radiation.
- Invasive ductal carcinoma - excision with sentinel lymph node biopsy (for staging)[2] and radiation.
- Positive sentinel node - systemic chemotherapy. (???)
IHC
Usual ductal hyperplasia (AKA FEHUT) vs. ADH/DCIS:[3][4]
- FEHUT: ER-low/CK5-high profile.
- ADH/DCIS: ER-high/CK5-low.
Where:
- ER-high = diffuse strong staining in >90% of cells.
- CK5-high = mosaic pattern of staining in >20% of cells
- CK5-low = absent or staining in <20% of cells.
Atypical ductal hyperplasia
- Abbreviated ADH.
Ductal carcinoma in situ
- Abbreviated DCIS.
General
- Diagnosis based on nuclear abnormalities and/or architecture.
- Low-grade DCIS does not have a malignant cytology.
- It is typically picked-up during radiologic screening.
Microscopic
Features:
- Architectural changes:
- Equal spacing of cells - "cookie cutter" look.
- Cells line-up along lumen/glandular spaces - form "Roman briges".
- Architecture suggestive of DCIS - see Subtypes of DCIS.
- Nuclear changes:
- Nuclear enlargement - at least 2-3x size of RBC - key feature.
- Compared to RBCs to grade DCIS - see Grading DCIS.
- Compare sizes of nuclei if you cannot find RBCs.
- Compared to RBCs to grade DCIS - see Grading DCIS.
- Nuclear pleomorphism - important feature.
- Nuclear enlargement - at least 2-3x size of RBC - key feature.
- +/-Mitoses.
Note:
- Apocrine changes of cytoplasm -- several sets of criteria exist -- any of the following:
Subtypes of DCIS
The subtypes are based on architecture.
Note:
- Comedonecrosis used to be considered a separate subtype. Necrosis is seen most often in the context of solid ductal carcinoma in situ.
Solid ductal carcinoma in situ
Features:
- Sheet of cells fills the duct
- No spaces between cells.

Breast - Ductal carcinoma in situ - Solid variant- Intermediate grade - Medium power (SKB)

Breast - Ductal carcinoma in situ - Solid variant- Intermediate grade - Low power (SKB)
Breast - Ductal carcinoma in situ - Solid variant - Medium power (SKB)

Breast - Ductal carcinoma in situ - Solid variant - Comedonecrosis (SKB)

Breast - Ductal carcinoma in situ - Solid variant - Comedonecrosis (SKB)





DDx:
- LCIS.
- May show dyscohesion
- More monomorphic population of cells
Cribriform ductal carcinoma in situ
Features:
- Honeycomb-like appearance: circular holes.
- "Cookie cutter" appearance/"punched-out" appearance/"Roman bridges" -- cells surround the circular holes.

Breast - Ductal carcinoma in situ - cribriform varient - medium power (SKB)

Breast - Ductal carcinoma in situ - cribriform varient - medium power (SKB)


DDx:
- Collagenous spherulosis.
- Adenoid cystic carcinoma of the breast.
- Invasive cribriform carcinoma of the breast
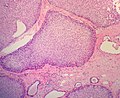
Papillary ductal carcinoma in situ
Features:
- Papillae with fibrovascular cores.
- Papillae lack a myoepithelial layer
- Papillae are lined by atypical cells.
- Papillae within a ductal space lined by myoepithelial cells.

Breast - Ductal carcinoma in situ - Papillary variant - low power (SKB)
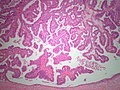
Breast - Ductal carcinoma in situ - Papillary variant - Medium power (SKB)


DDX:
- Intraductal papilloma
- Ductal carcinoma in situ arising within an intraductal papilloma
- Intracystic papillary breast carcinoma
- Invasive papillary breast carcinoma
Micropapillary ductal carcinoma in situ
Features:
- Small papillae without fibrovascular cores.
- Have "drum stick" shape.
DDx:

Breast - Ductal carcinoma in situ - micropapillary variant - Medium power - (SKB)

Breast - Ductal carcinoma in situ - micropapillary variant - High power - (SKB)
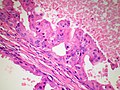
Breast - Ductal carcinoma in situ - Micropapillary type with apocrine features - High power - (SKB)



Grading DCIS
Graded 1-3 (low-high)[7] - compare lesional nuclei to one another.
- Grade 1:
- Nuclei 2-3x size of RBC.
- No necrosis.
- Grade 2:
- Nuclei 2-3x size of RBC.
- +/-Necrosis.
- Grade 3:
- Nuclei >3x size of RBC.
- Necrosis usually present.
Notes:
- It is often hard to find RBCs when you want 'em. DCIS is pleomorphic.
- If no RBCs are present to compare with compare the nuclei to one another.
- If you see nuclei >3x larger than their neigbour you're ready to call DCIS Grade 3.
Size criteria for low-grade DCIS
ADH is diagnosed if the lesion is small - specifically:[8][9]
- < Two membrane-bound spaces.
- < 2 mm extent. ‡
The treatment is similar; ADH and DCIS are both excised.
The differences are:
- DCIS is cancer, i.e. this has life insurance implications.
- Radiation treatment - DCIS is irradiated; ADH does not get radiation.
Notes:
- ‡ 3 mm is used in papillary lesions.[citation needed]
Micrometastasis in DCIS
Micrometastasis in DCIS - not significant.[10][11]
Lobular neoplasia
Overview
Includes:
- Atypical lobular hyperplasia (ALH).
- Lobular carcinoma in situ (LCIS).
- These entities (ALH, LCIS) are near identical from a histomorphologic perspective.
- The difference is extent of involvement:
- ALH <50% of terminal duct lobular unit (TDLU) is involved.
- LCIS >=50% of TDLU is involved.
Atypical lobular hyperplasia
- Abbreviated ALH.
General
- May occur with ductal involvement by cells of atypical lobular hyperplasia (abbreviated DIALH).[12]
- ALH with DIALH has a risk of developing breast cancer that is similar to LCIS.
Microscopic
Features:
- Extent criterium: <50% of terminal duct lobular unit (TDLU) is involved.
- See lobular carcinoma in situ for details.
DDx:
IHC
- E-cadherin -ve or incomplete membrane staining.
Lobular carcinoma in situ
- Abbreviated LCIS.
General
- Management is currently some matter of debate.
- Not detected radiologically - it is an incidental pathologic finding.
- The precursor to invasive ductal carcinoma of the breast.
Microscopic
Features[15][16] - memory device ABCDEF:
- Atypia minimal - usually.
- Relatively small ~1-2x size lymphocyte.
- Borders of cells distinct/visible - dyscohesive.
- Clear cytoplasm (focal).
- May have a signet ring cell-like appearance.
- Distend duct.
- Eccentric nucleus, usu. round.
- Filled ducts.
- No luminal spaces - key feature.
- Partially filled ducts are not LCIS.
- No luminal spaces - key feature.
DDx:
Images:
Subclassification[16]
- Non-PLCIS.
- Type A.
- Nucleus 1-1.5x lymphocyte.
- No nucleolus.
- Type B.
- Nucleus ~2x lymphocyte.
- Nucleolus present.
- Type A.
- PLCIS (pleomorphic lobular carcinoma in situ).
DDx:
- Low-grade DCIS.
- High-grade DCIS for pleomorphic lobular carcinoma in situ.
- Atypical lobular hyperplasia.
IHC
- E-cadherin -ve or incomplete membrane staining.
- p120 catenin +ve cytoplasmic.[17]
- Membranous staining in DCIS.
See also
References
- ↑ O'Malley, Frances P.; Pinder, Sarah E. (2006). Breast Pathology: A Volume in Foundations in Diagnostic Pathology series (1st ed.). Churchill Livingstone. pp. 167-8. ISBN 978-0443066801.
- ↑ Sentinel Lymph Node Biopsy: What Breast Cancer Patients Need to Know. cancernews.com. URL: http://www.cancernews.com/data/Article/202.asp. Accessed on: 9 October 2009.
- ↑ Rabban, JT.; Koerner, FC.; Lerwill, MF. (Jul 2006). "Solid papillary ductal carcinoma in situ versus usual ductal hyperplasia in the breast: a potentially difficult distinction resolved by cytokeratin 5/6.". Hum Pathol 37 (7): 787-93. doi:10.1016/j.humpath.2006.02.016. PMID 16784976.
- ↑ Grin, A.; O'Malley, FP.; Mulligan, AM. (Nov 2009). "Cytokeratin 5 and estrogen receptor immunohistochemistry as a useful adjunct in identifying atypical papillary lesions on breast needle core biopsy.". Am J Surg Pathol 33 (11): 1615-23. doi:10.1097/PAS.0b013e3181aec446. PMID 19675450.
- ↑ URL: http://surgpathcriteria.stanford.edu/breast/dcis/apocrinedcis.html. Accessed on: 4 August 2011.
- ↑ 6.0 6.1 O'Malley, FP.; Bane, A. (Jan 2008). "An update on apocrine lesions of the breast.". Histopathology 52 (1): 3-10. doi:10.1111/j.1365-2559.2007.02888.x. PMID 18171412.
- ↑ URL: http://surgpathcriteria.stanford.edu/breast/dcis/. Accessed on: 4 August 2011.
- ↑ O'Malley, Frances P.; Pinder, Sarah E. (2006). Breast Pathology: A Volume in Foundations in Diagnostic Pathology series (1st ed.). Churchill Livingstone. pp. 168. ISBN 978-0443066801.
- ↑ Tadrous, Paul.J. Diagnostic Criteria Handbook in Histopathology: A Surgical Pathology Vade Mecum (1st ed.). Wiley. pp. 258. ISBN 978-0470519035.
- ↑ Lara, JF.; Young, SM.; Velilla, RE.; Santoro, EJ.; Templeton, SF. (Nov 2003). "The relevance of occult axillary micrometastasis in ductal carcinoma in situ: a clinicopathologic study with long-term follow-up.". Cancer 98 (10): 2105-13. doi:10.1002/cncr.11761. PMID 14601079.
- ↑ Broekhuizen, LN.; Wijsman, JH.; Peterse, JL.; Rutgers, EJ. (Jun 2006). "The incidence and significance of micrometastases in lymph nodes of patients with ductal carcinoma in situ and T1a carcinoma of the breast.". Eur J Surg Oncol 32 (5): 502-6. doi:10.1016/j.ejso.2006.02.006. PMID 16569492.
- ↑ Page, DL.; Dupont, WD.; Rogers, LW. (Feb 1988). "Ductal involvement by cells of atypical lobular hyperplasia in the breast: a long-term follow-up study of cancer risk.". Hum Pathol 19 (2): 201-7. PMID 3343034.
- ↑ 13.0 13.1 Chester, R.; Bokinni, O.; Ahmed, I.; Kasem, A. (Nov 2015). "UK national survey of management of breast lobular carcinoma in situ.". Ann R Coll Surg Engl 97 (8): 574-7. doi:10.1308/rcsann.2015.0037. PMID 26492902.
- ↑ O'Neil, M.; Madan, R.; Tawfik, OW.; Thomas, PA.; Fan, F. (Aug 2010). "Lobular carcinoma in situ/atypical lobular hyperplasia on breast needle biopsies: does it warrant surgical excisional biopsy? A study of 27 cases.". Ann Diagn Pathol 14 (4): 251-5. doi:10.1016/j.anndiagpath.2010.04.002. PMID 20637429.
- ↑ Weedman Molavi, Diana (2008). The Practice of Surgical Pathology: A Beginner's Guide to the Diagnostic Process (1st ed.). Springer. pp. 188. ISBN 978-0387744858.
- ↑ 16.0 16.1 O'Malley, Frances P.; Pinder, Sarah E. (2006). Breast Pathology: A Volume in Foundations in Diagnostic Pathology series (1st ed.). Churchill Livingstone. pp. 170. ISBN 978-0443066801.
- ↑ Sarrió, D.; Pérez-Mies, B.; Hardisson, D.; Moreno-Bueno, G.; Suárez, A.; Cano, A.; Martín-Pérez, J.; Gamallo, C. et al. (Apr 2004). "Cytoplasmic localization of p120ctn and E-cadherin loss characterize lobular breast carcinoma from preinvasive to metastatic lesions.". Oncogene 23 (19): 3272-83. doi:10.1038/sj.onc.1207439. PMID 15077190.