Difference between revisions of "Disordered proliferative endometrium"
Jump to navigation
Jump to search
(split out) |
|||
| Line 6: | Line 6: | ||
Treatment: | Treatment: | ||
*Progesterone<ref name=pmid16873562/> versus observation.<ref name=pmid17090792>{{Cite journal | last1 = Ely | first1 = JW. | last2 = Kennedy | first2 = CM. | last3 = Clark | first3 = EC. | last4 = Bowdler | first4 = NC. | title = Abnormal uterine bleeding: a management algorithm. | journal = J Am Board Fam Med | volume = 19 | issue = 6 | pages = 590-602 | month = | year = | doi = | PMID = 17090792 | url = http://www.jabfm.org/content/19/6/590.full }}</ref> | *Progesterone<ref name=pmid16873562>{{Cite journal | last1 = McCluggage | first1 = WG. | title = My approach to the interpretation of endometrial biopsies and curettings. | journal = J Clin Pathol | volume = 59 | issue = 8 | pages = 801-12 | month = Aug | year = 2006 | doi = 10.1136/jcp.2005.029702 | PMID = 16873562 }}</ref> versus observation.<ref name=pmid17090792>{{Cite journal | last1 = Ely | first1 = JW. | last2 = Kennedy | first2 = CM. | last3 = Clark | first3 = EC. | last4 = Bowdler | first4 = NC. | title = Abnormal uterine bleeding: a management algorithm. | journal = J Am Board Fam Med | volume = 19 | issue = 6 | pages = 590-602 | month = | year = | doi = | PMID = 17090792 | url = http://www.jabfm.org/content/19/6/590.full }}</ref> | ||
Image: | Image: | ||
Revision as of 01:13, 1 May 2014
Disordered proliferative endometrium, abbreviated DPE, is an abnormal endometrial finding with some features of simple endometrial hyperplasia.
General
- Association: anovulation.
- Benign - can be grouped with normal.[1]
Treatment:
Image:
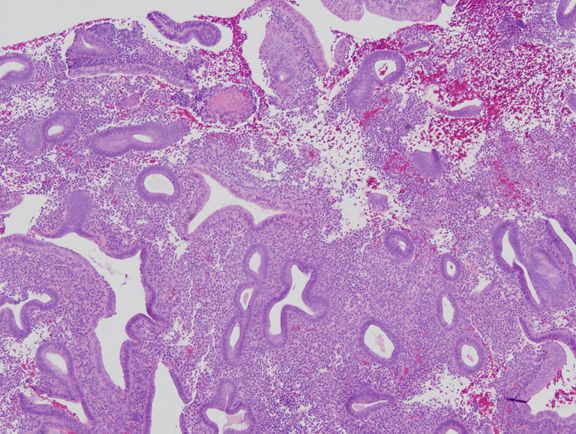
Microscopic
Features:[4]
- Proliferative type endometrium with:
- Cystic dilation of glands focally that do not have (glandular) secretions - key feature.
- Glands >2x normal size - usually 3-4x normal.
- Irregular shape, e.g. gland contour has inflection points.
- Greater than fours glands involved (dilated).
- Cystic dilation of glands focally that do not have (glandular) secretions - key feature.
- +/-Stromal condensation -- balls of stromal tissue, aka "blue balls" (due to breakdown of endometrium).
Notes:
- Dilated glands often have tubal metaplasia.[citation needed]
- Eosinophilic syncytial metaplasia - common.
- Features: abundant eosinophilic cytoplasm, mild nuclear atypia +/-loss of nuclear stratification, no mitoses).
DDx:
- Proliferative phase endometrium.
- Glands: straight, tubular, tall pseudostratified columnar cells, mitotic figures, no vacuolation, no mucus secretion, abundant mitoses.
- Stroma: cellular, stroma (spindle cells), mitoses.
- Simple endometrial hyperplasia without atypia - architectural atypia diffuse.
- Benign endometrial polyp.
Images
www:

Endometrial stromal condensation - high mag. (WC/Nephron)

{kind=link}
Sign out
ENDOMETRIUM, BIOPSY: - DISORDERED PROLIFERATIVE ENDOMETRIUM.
With endocervix
ENDOMETRIUM, BIOPSY: - DISORDERED PROLIFERATIVE ENDOMETRIUM. - BENIGN ENDOCERVICAL MUCOSA.
Waffle a bit
ENDOMETRIUM, BIOPSY: - COMPATIBLE WITH DISORDERED PROLIFERATIVE ENDOMETRIUM (FRAGMENTS OF PROLIFERATIVE ENDOMETRIUM WITH EVIDENCE OF SHEDDING AND VERY RARE GLAND DILATION). - VERY SCANT STRIPPED ENDOCERVICAL EPITHELIUM WITHOUT APPARENT PATHOLOGY. - NEGATIVE FOR ENDOMETRIAL HYPERPLASIA. - NEGATIVE FOR MALIGNANCY.
ENDOMETRIUM, CURETTAGE: - PROLIFERATIVE ENDOMETRIUM, FOCALLY WITH GLAND DILATION AND SMALL BLOOD VESSELS, SEE COMMENT. - NEGATIVE FOR HYPERPLASIA AND NEGATIVE FOR MALIGNANCY. COMMENT: A fibrotic stroma is not present. The findings may represent a remnant of the previously excised endometrial polyp or disordered proliferative endometrium. Follow-up is suggested.
Micro
The sections show a well-sampled endometrium. Mitotic figures are identified within the glands and stroma. Irregular, moderately enlarged glands are seen (only) in one of several fragments; most of the endometrial glands are round, regular and small.
No stromal condensation is apparent. No secretions are in the glands.
There are no back-to-back glands. No nuclear atypia is apparent. No thick-walled blood vessels are apparent.
See also
References
- ↑ Sherman, ME.; Ronnett, BM.; Ioffe, OB.; Richesson, DA.; Rush, BB.; Glass, AG.; Chatterjee, N.; Duggan, MA. et al. (Jul 2008). "Reproducibility of biopsy diagnoses of endometrial hyperplasia: evidence supporting a simplified classification.". Int J Gynecol Pathol 27 (3): 318-25. doi:10.1097/PGP.0b013e3181659167. PMID 18580308.
- ↑ McCluggage, WG. (Aug 2006). "My approach to the interpretation of endometrial biopsies and curettings.". J Clin Pathol 59 (8): 801-12. doi:10.1136/jcp.2005.029702. PMID 16873562.
- ↑ 3.0 3.1 Ely, JW.; Kennedy, CM.; Clark, EC.; Bowdler, NC.. "Abnormal uterine bleeding: a management algorithm.". J Am Board Fam Med 19 (6): 590-602. PMID 17090792. http://www.jabfm.org/content/19/6/590.full.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 1080 and 1082. ISBN 0-7216-0187-1.
- ↑ URL: http://www.glowm.com/index.html?p=glowm.cml/section_view&articleid=235. Accessed on: 11 December 2012.