Difference between revisions of "Dermal cysts"
(→Epidermal inclusion cyst: split-out) |
|||
| Line 55: | Line 55: | ||
==Epidermal inclusion cyst== | ==Epidermal inclusion cyst== | ||
{{Main|Epidermal inclusion cyst}} | |||
==Pilar cyst== | ==Pilar cyst== | ||
Revision as of 02:08, 31 October 2013
Dermal cysts, also skin cysts, are common in dermatopathology. Dermatopathologists can diagnose 'em.
Overview
Common types:[1]
- Epidermal cyst (sebaceous cyst) -- most common.
- Pilar (trichilemmal) cyst.
- Dermoid cyst.
- Ganglion cyst.
- Milicem.
Epidermal necrosis
- This may be cystic. It is covered in the epidermal necrosis article, which covers erythema multiforme, Steven-Johnson syndrome and toxic epidermal necrolysis.
Common cysts
Venous lake
General
- Dilated vein.
Clinical:
- Blanch with pressure.[2]
Gross
- Purple/blue spot.
Images:
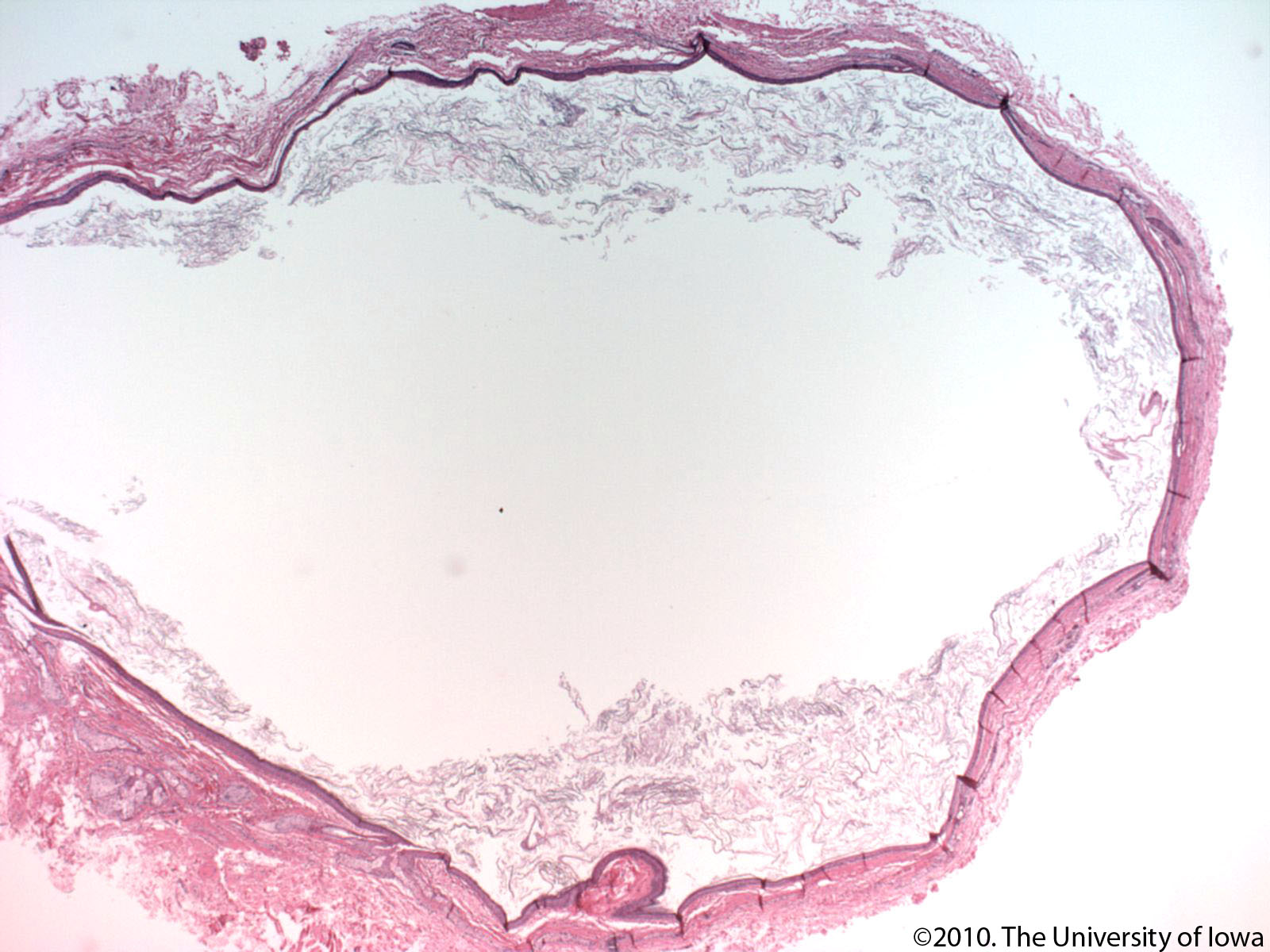
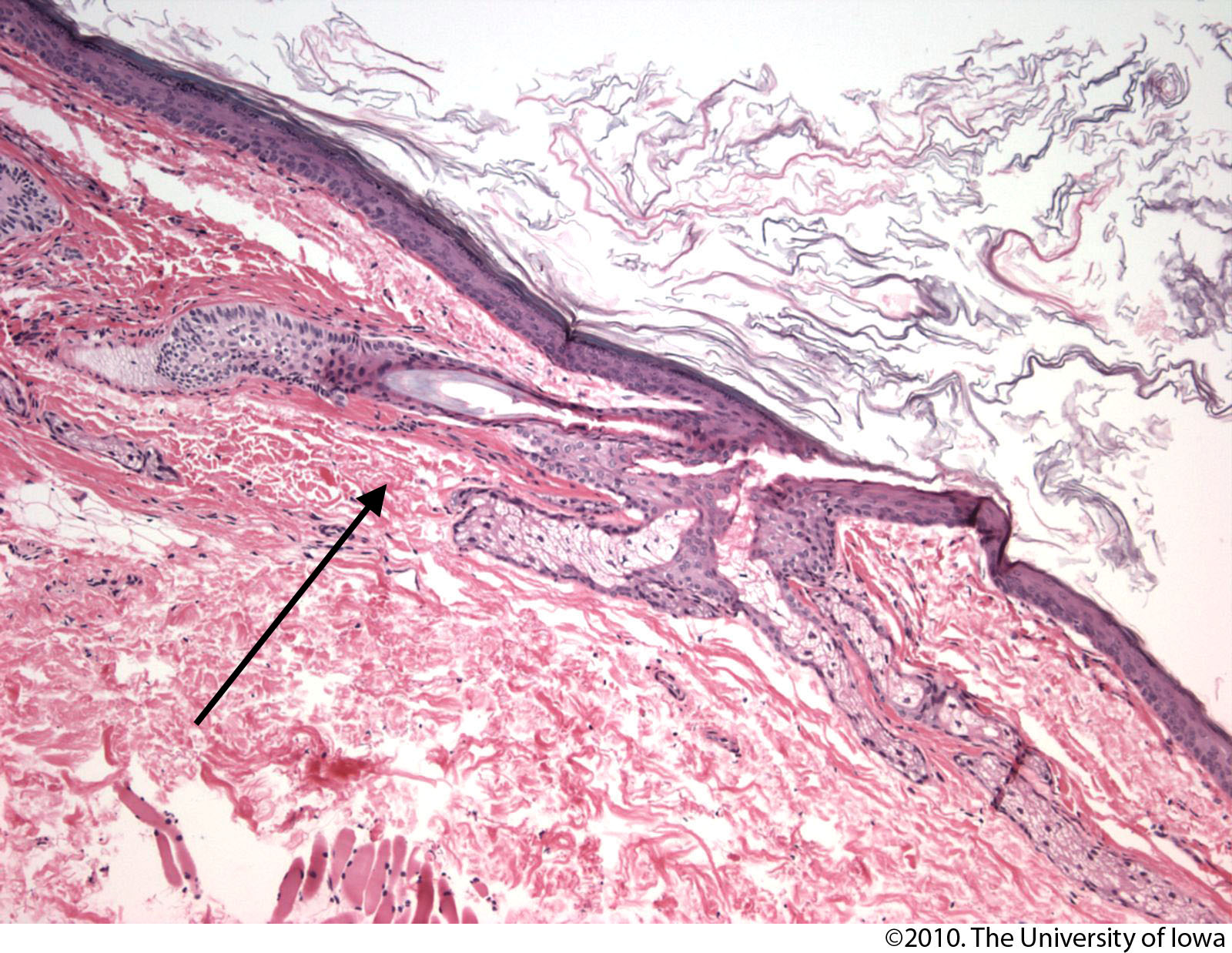
Microscopic
Features:[4]
- Lined by endothelium.
- Blood in lumen.
- +/-Fibrin in lumen.
- +/-Solar elastosis - very common.[5]
DDx:
- Angiokeratoma.
- Ectatic superficial dermal vessels.
- Irregular acanthosis.
- Longer rete ridges.
- Cherry hemangioma.[5]
Images:
- Venous lake (jhmi.edu).[3]
- Venous lake (dermpedia.org).[6]
- Venous lake (surgical pathologyatlas.com).
Sign out
SKIN LESION, RIGHT CHEEK, BIOPSY: - VENOUS LAKE. - SOLAR ELASTOSIS. - NEGATIVE FOR NEVUS.
Epidermal inclusion cyst
Pilar cyst
- AKA trichilemmal cyst.
General
- Very common.
Gross
- Classic location: head ~90%.[7]
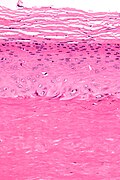
Microscopic
Features:[8]
- Keratin.
- Cyst lining:
- Has no granular layer - key feature.
- Keratohyaline granules (as seen in the granular layer) may be seen focally.
- Inner most cyst lining cells are large cells with abundant eosinophilic cytoplasm.
- Has no granular layer - key feature.
DDx:
- Epidermal cyst - has a granular layer.
Images

Trichilemmal cyst - intermed. mag. (WC)
Trichilemmal cyst - very high mag. (WC)


www:
Sign out
SCALP (CYST), EXCISION: - TRICHILEMMAL CYST (PILAR CYST).
SKIN CYST, LEFT FLANK, EXCISION: - TRICHILEMMAL CYST (PILAR CYST).
SCALP (CYST), ANTERIOR, EXCISION: - TRICHILEMMAL CYST (PILAR CYST), RUPTURED.
Micro
The sections show a cyst that is lined by squamous epithelium without a granular layer. Focally, keratohyaline granules are seen in the cyst lining cells. The innermost cyst lining cells are large and have abundant eosinophilic cytoplasm. The cyst contains keratin.
Dermoid cyst
General
- Benign.
- Congenital choristomas.[9]
- May be found in the ovary.
Microscopic
- Cyst lined by normal (keratinized) skin with adnexal structure (hair follicles, sweat glands, sebaceous glands).
DDx:
- Epidermal cyst - no adnexal structures.
Images:
Sign out
OVARY AND UTERINE TUBE, LEFT, UNILATERAL SALPINGO-OOPHORECTOMY: - MATURE TERATOMA. - UTERINE TUBE WITHIN NORMAL LIMITS. - NEGATIVE FOR MALIGNANCY.
Pilonidal cyst
General
- Benign.
- Young adults (late teens, early twenties) - usu. men.[12]
Gross
- Usually at gluteal folds.
- Uncommon: axilla, genital region, umbilicus, scalp.[13]
Microscopic
Features:[13]
- Cyst or pseudocyst into the deep dermis.
- May be lined by squamous epithelium with inflammation +/-pseudoepitheliomatous hyperplasia.
- Neutrophils.
- Granulomatous inflammation.
DDx:
- Squamous cell carcinoma of the skin with inflammation.[14]
- Infection.
Sign out
SKIN LESION (PILONIDAL SINUS), EXCISION: - PILONIDAL SINUS. - NEGATIVE FOR MALIGNANCY.
Micro
The section shows hair-bearing skin with a deep sinus tract containing large clusters of neutrophils, abundant plasma cells, hemosiderin-laden macrophages, eosinophils and multinucleated giant cells. The core of the lesion is, focally, well-vascularized. At the edge of the lesion is fibrotic tissue with plump fibroblasts. Benign, fibrofatty tissue with scant inflammation completely surrounds the tract, in the plane of section; however, it is focally fragmented. There is no squamous lining within the sinus. No nuclear atypia is identified.
Alternate
The section shows hair-bearing skin with a deep sinus containing large clusters of neutrophils, abundant plasma cells, hemosiderin-laden macrophages and multinucleated giant cells. Benign fibrofatty tissue with scant inflammation completely surrounds the lesion in the plane of section. There is no squamous lining within the sinus. No nuclear atypia is identified.
Less common
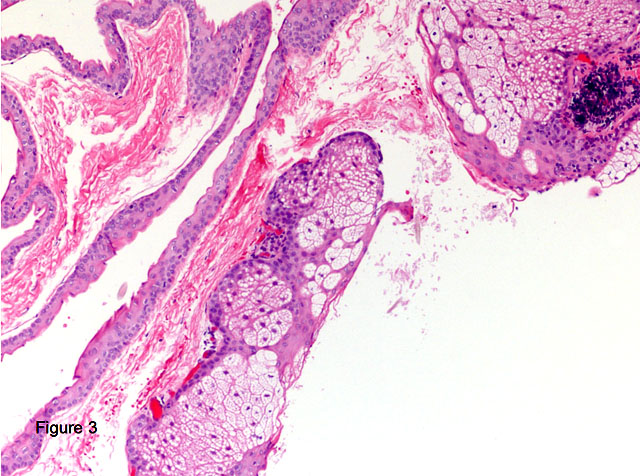
Steatocystoma
General
- Benign.
- Typically adults.
- Usually on the trunk.
- May be genetic; known as steatocystoma multiplex.[15]
- Classically autosomal dominant.[16]
Microscopic
Features:[17]
- Cyst lined by squamous epithelium with:
- Corrugated eosinophilic lining - key feature.
- Similar appearance to compact keratin (hyperkeratosis).
- Described as a hyaline cuticle.[18]
- No granular cell layer.
- Corrugated eosinophilic lining - key feature.
Images
Steatocystoma. (WC)

Steatocystoma - low mag. (WC/Nephron)

Steatocystoma - intermed. mag. (WC/Nephron)



{kind=link}
{kind=link}
www:
{kind=link}
Digital mucous cyst
General
- Dome-shaped papule.
Microscopic
Features:[20]
- Mucous in superficial dermis - key feature.
- No epithelial lining; it is a pseudocyst.
Note:
- Mucin = glycolated proteins; may be part of mucous.
- Mucous = slippery secretion.
DDx:
Images:
{kind=link}
{kind=link}
Sign out
LESION, LEFT INDEX FINGER, EXCISION: - DIGITAL MUCOUS CYST.
Apocrine cystadenoma
General
- Uncommon.
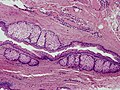
Microscopic
Features:[24]
- Multiloculated.
- Apocrine differentiation: columnar epithelium +/- apical snouts.
- Solid areas of epithelial proliferation.
- Papillary projections into the cyst.
Images:
See also
References
- ↑ Greenwald, J.; Heng, M. (2007). Toronto Notes for Medical Students 2007 (2007 ed.). The Toronto Notes Inc. for Medical Students Inc.. pp. D5. ISBN 978-0968592878.
- ↑ URL: http://dermatlas.med.jhmi.edu/derm/IndexDisplay.cfm?ImageID=-969536424. Accessed on: 13 August 2012.
- ↑ 3.0 3.1 3.2 URL: http://dermatlas.med.jhmi.edu/derm/result.cfm?Diagnosis=605386295. Accessed on: 13 August 2012.
- ↑ Weedon's Skin Pathology. 3rd Ed. P.895.
- ↑ 5.0 5.1 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 551. ISBN 978-0443066542.
- ↑ URL: http://www.dermpedia.org/case/70-year-old-woman-with-nose-lesion. Accessed on: 21 June 2013.
- ↑ URL: http://emedicine.medscape.com/article/1058907-overview. Accessed on: 15 April 2012.
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 309. ISBN 978-0443066542.
- ↑ 9.0 9.1 9.2 Gandhi N, Syed NA, Alen R. Dermoid Cyst. EyeRounds.org. posted July 26, 2010; Available from: http://www.EyeRounds.org/cases/115-dermoid-cyst.htm. Accessed on: 22 September 2011.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 596. ISBN 978-1416054542.
- ↑ URL: http://emedicine.medscape.com/article/788127-overview. Accessed on: 10 September 2012.
- ↑ URL: http://www.nhs.uk/conditions/Pilonidal-sinus/Pages/Introduction.aspx. Accessed on: 10 September 2012.
- ↑ 13.0 13.1 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 326. ISBN 978-0443066542.
- ↑ Chatzis, I.; Noussios, G.; Katsourakis, A.; Chatzitheoklitos, E.. "Squamous cell carcinoma related to long standing pilonidal-disease.". Eur J Dermatol 19 (4): 408-9. doi:10.1684/ejd.2009.0705. PMID 19482585.
- ↑ Online 'Mendelian Inheritance in Man' (OMIM) 184500
- ↑ URL: http://path.upmc.edu/cases/case674/dx.html. Accessed on: 29 January 2012.
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 312. ISBN 978-0443066542.
- ↑ URL: http://path.upmc.edu/cases/case674/dx.html. Accessed on: 29 January 2012.
- ↑ URL: http://path.upmc.edu/cases/case674.html. Accessed on: 29 January 2012.
- ↑ 20.0 20.1 20.2 20.3 URL: http://www.dermpedia.org/dermpedia-textbook/digital-mucous-myxoid-cyst. Accessed on: 17 January 2012.
- ↑ URL: http://dictionary.reference.com/browse/mucous. Accessed on: 8 January 2012.
- ↑ URL: http://dictionary.reference.com/browse/mucus. Accessed on: 8 January 2012.
- ↑ URL: http://www.dermpedia.org/case/digital-mucous-cyst-ganglion-type. Accessed on: 5 July 2013.
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 316. ISBN 978-0443066542.