Difference between revisions of "Haematopathology"
m (→Subtypes: fix ref) |
|||
| Line 271: | Line 271: | ||
***Dimensions: approx. 0.5-1 x 4-6 micrometres. | ***Dimensions: approx. 0.5-1 x 4-6 micrometres. | ||
**Images: [http://en.wikipedia.org/wiki/File:Auer_rods.PNG Auer rods (WP)], [http://www.healthsystem.virginia.edu/internet/hematology/HessImages/Acute-myelogenous-leukemia-M4-100x-Auer-rods-website-arrow.jpg Auer rods (virginia.edu)]. | **Images: [http://en.wikipedia.org/wiki/File:Auer_rods.PNG Auer rods (WP)], [http://www.healthsystem.virginia.edu/internet/hematology/HessImages/Acute-myelogenous-leukemia-M4-100x-Auer-rods-website-arrow.jpg Auer rods (virginia.edu)]. | ||
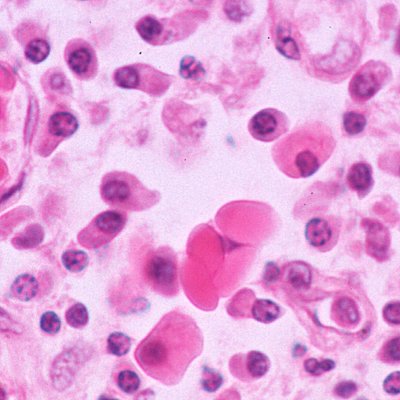
==Angioimmunoblastic T-cell lymphoma== | |||
===Microscopic=== | |||
Features: | |||
*Clear cytoplasm. | |||
*"Empty" sinus; subcapsular sinuses "open". | |||
===IHC=== | |||
*CD7 -ve. | |||
*CD20 +ve. | |||
*TIA-1 -ve. | |||
==Anaplastic large cell lymphoma== | ==Anaplastic large cell lymphoma== | ||
Revision as of 17:47, 6 August 2010
Understanding of haematopathology is important in anatomical pathology, as haematologic malignancies are often in the (clinical) differential diagnosis and may mimic small blue round cell tumours or lobular breast carcinoma.
The lymph node is discussed below; however, details are covered in the lymph node article and lymph node pathology article.
Bone marrow
Bone marrows are important for understanding haematopathology. They are dealt with in the bone article.
Normal lymph node
Normal (clinical)
- Round.
- "Soft".
- Mobile.
Pathologic (clinical) - associations
- Rubbery = suggestive of lymphoma.
- Fixed (immobile) = suggestive of cancer.
- Tender (hurts when ya touch it) = suggestive of infection.
Radiologic & clinical
- Elongated = may be cancer.
- "Large" = could be cancer or infection.
Malignant - statistical associations
Nodes with metstases tend to be:
- Hard.
- Ellipical (as opposed to circular) on section.
- "Large".
- May be immobile (fixed to a surrounding structure).
Note:
- "Large" depends on the location in the body.
Gross pathologic exam
Normal:
- Firm (relative to adipose tissue).
- Glistening surface when cut.
Pathologic:
- White lesions, espically irregular = suggestive of carcinoma.
- White, glistening, with lobulated surface - "fish flesh" = suggestive of lymphoma.
- Subtle lobulation (~1 mm) on section suggestive of follicular lymphoma.[1]
Microscopic
The microscopic lymph node architecture in described the lymph node article, along with B cell maturation and lymph node cell types.
The cells of the lymph node:
- Germinal center:
- Centrocytes - cleaved nucleus.
- Centroblasts - large dark, mitotically active, medullary aspect of germinal center.
- Tingible body macrophages.
- Follicular dendritic cells.
- Paracortex:
- T lymphocytes.
- Interdigitating dendritic cells.
- Mantle zone:
- Immunoblasts (Memory B cells) - small lymphocytes.
- Medulla:
- B lymphocytes.
- Plasma cells.
Heparin-induced thrombocytopenia
- Thrombocytopenia due to heparin.[2]
Classification:
- Type 1 - in first two days of exposure - considered non-immune and considered not to be serious.
- Type 2 - in the first 4-10 days - considered serious.
Diagnosis (simplified):
- 50% decline in platelets - within 4-10 days of starting heparin.
- HIT assay - several exist.[3]
Lymphoma classification
Lymphomas can be divided into:
- Hodgkin's lymphoma.
- Non-Hodgkin's lymphoma (NHL).
Other categorizations:
- T cell lymphomas (rare).
- B cell lymphomas (more common).
Two most common NHLs:
- Follicular lymphoma (FL).
- Diffuse large B-cell lymphoma (DLBCL).
Lymphoma as a med student
- Acute lymphoid leukemia (ALL) - predominantly in smALL people, i.e. children.
- Acute myeloid leukemia (AML).
- Chronic myeloid leukemia (CML).
- Chronic lymphoid leukemia (CLL) - relatively good prognosis.
Histology
- Lymphomas = cells look discohesive, may be difficult to differentiate from poor differentiated carcinoma.
- Auer rods = Acute myeloid leukemia.
- Granular cytoplasmic rod (0.5-1 x4-6 micrometres).
- Reed-Sternberg cells = Hodgkin's lymphoma.
- Large cell - very large nucleus.
- Classically binucleated.
- Large cell - very large nucleus.
- Russell bodies = Plasmacytoma (+others).
IHC
- CD45+.
- AKA common lymphocyte antigen.
- Useful to differentiate from carcinomas (e.g. small cell carcinoma).
- CD3 -- T cell marker (all T cells).
- CD4 -- subset of T cells.
- CD8 -- subset of T cells.
- CD20 -- B cell marker.
- CD19 -- B cell marker - used for flow cytometry.
- CD10 -- follicule center.
- CD30 -- Hodgkin's lymphoma (most sensitive).
- CD23 -- follicular dendritic cells.
- CD21 -- follicular dendritic cells.
Hodgkin's lymphoma
General
- Abbreviated HL.
Microscopic
By definition, HL has Reed-Sternberg cells (RSCs).
Classical HL
Features (classic HL):
- Reed-Sternberg cell.
- Large binucleated cell.
- Macronucleolus - approximately the size of a RBC (~8 micrometers).
- Well-defined cell border.
Images (classic HL):
- HL mixed cellularity - cytology (WC).
- HL mixed cellularity - cytology (WC).
- HL mixed cellularity (WC).
{kind=link}
{kind=link}
{kind=link}
Subtypes
There are four CHL subtypes:[5]
- Nodular sclerosis CHL - ~70% of CHL.
- Mixed cellular background - T cell, plasma cells, eosinophils, neutrophils and histiocytes.
- Nodular sclerosing fibrosis - thick strands fibrosis.
- Mixed cellularity CHL - ~20-25% of CHL.
- Like nodular sclerosis - but no fibrosis.
- Lymphocyte-rich CHL - rare.
- T lymphocytes only (no mix of cells).
- Lymphocyte-depleted CHL - rare.
- Assoc. with HIV infection.
Memory device:
- The subtypes prevalence is in reverse alphabetical order.
Nodular lymphocyte-predominant HL
Features (nodular lymphocyte-predominant Hodgkin's lymphoma):
- Lymphocytic & histiocytic cell (L&H cell)[6] - variant of RSC:
- Cells (relatively) small (compared to classic RSCs).
- Lobulated nucleus - key feature.
- Small nucleoli.
Image (NLPHL):
Follicular lymphoma
- A very common type of lymphoma.
- Express Bcl-2.[7]
Microscopic
Features:
- Abundant abnormal lymphoid follicles.
IHC
Features:[7]
- CD10+/-.
- CD5-.
- CD23-/+.
- CD43-.
- CD11c-.
Molecular
- t(14;18)(q32;q21)/IGH-BCL2 in 70-95% of cases.[7]
- Should not be confused with t(14;18)(q32;q21)/IGH-MALT1 seen in MALT lymphomas.[8]
Diffuse large B-cell lymphoma
- Abbreviated DLBCL.
Microscopic
Features:[9]
- Large cells -- 4-5 times the diameter of a small lymphocytes.
- Typically have marked cell-to-cell variation in size and shape.
- Cytoplasm usu. basophilic and moderate in abundance.
- +/-Prominent nucleoli, may be peripheral and/or multiple.
Notes:
- Large bizarre cells can occasionally mimic Reed-Sternberg cells, seen in Hodgkin lymphoma.
Burkitt's lymphoma
General
- Abbreviated BL.
- Extremely high proliferative rate & rate of apoptosis.
Subtypes
- Three subtypes recognized:[10]
- Endemic:
- Found in Africa.
- EBV (Epstein-Barr virus) associated.[10]
- Non-endemic:
- Typical of the BL seen in the western world; EBV negative.
- Immunodeficiency associated:
- Associated with HIV infection.
Pathophysiology
- Origin cell: germinal centre B cells (favoured) vs. memory B cells.[10]
- Common translocation t(8;14).[10]
Cytologic definition
- t(8;14) (q24;q32) translocation + a few variants or c-myc rearrangement.[10]
Histology
- "Starry-sky pattern".
- The stars in the pattern are: tingible-bodies laden macrophages.
- Tingible-bodies macrophages = macrophages containing dead body of apoptotic tumor cells.
- The stars in the pattern are: tingible-bodies laden macrophages.
- Tumour cells:[10]
- Medium size.
- Round nuclei.
- Multiple nucleoli.
- Relatively abundant cytoplasm.
Image: Starry-sky pattern - Ed Uthman (www.wikipedia.org).
{kind=link}
Plasmacytoma
General
- Malignancy derived from the plasma cells.
- Histologic component of multiple myeloma; to diagnose multiple myeloma other (non-pathology) criteria are needed.
- Prognosis: poor.
Microscopic
- Cells with "clock face" nuclei.
- Russell bodies:
- Eosinophilic, large (10-15 micrometres), homogenous immunoglobulin-containing inclusions.
- Dutcher bodies - intranuclear crystalline rods.
- Dutcher bodies are PAS stain +ve.[11]
- Image Dutcher bodies (hematologylibrary.org).
- Prominent perinuclear hof - crescent shaped lucency at the nuclear membrane (due to large Golgi apparatus).
{kind=link}
{kind=link}
{kind=link}
Images: Various images (hematologylibrary.org).
DDx:
- Neuroendocrine carcinoma - nucleus often has a plasmacytoid (plasma cell-like) appearance.
Acute myeloid leukemia
General
- May afflicits young adult.
- Males>females.
Complications
- Chloroma - soft tissue mass.
- Leukostasis.
- Occurs - lungs and brain.[12]
- Hyperviscosity syndrome.
- Spontaneous bleeding with low platelet counts.
Classification
There are two classifications:
- FAB (French-American-British) - based on histologic appearance/maturation.
- WHO classification.
Histology
- Auer rods - not required to diagnose.[13]
- Cytoplasmic granular rods in blast cells.
- Dimensions: approx. 0.5-1 x 4-6 micrometres.
- Images: Auer rods (WP), Auer rods (virginia.edu).
- Cytoplasmic granular rods in blast cells.
{kind=link}
{kind=link}
Angioimmunoblastic T-cell lymphoma
Microscopic
Features:
- Clear cytoplasm.
- "Empty" sinus; subcapsular sinuses "open".
IHC
- CD7 -ve.
- CD20 +ve.
- TIA-1 -ve.
Anaplastic large cell lymphoma
General
- Abbreviated ALCL.
- May look a lot like a carcinoma.
- Often subcapsular in LNs.
- Usually T-cell derived.
- Alk IHC:
- +ve = good prognosis.
- -ve = bad prognosis.
DDx:
- Hodgkin's lymphoma.
Microscopic
Features:
- Large cells with eosinophilic cytoplasm.
- Usu. appear cohesive.
- May be subcapsular.
- Large multinucleated cell - "wreath cell" - key feature.
IHC
Features:
- Variable CD30 +ve. (???)
- CD45 +ve. (???)
Table of B-cell lymphoma
Small cell lymphomas:
| Name | Location | Size of cells | IHC | Translocations | Clinical | Other |
|---|---|---|---|---|---|---|
| Follicular lymphoma | Follicle | Small, centrocytes, centroblasts | CD10+, bcl-6+[14] | t(14,18) | Clinical ? | Other ? |
| Mantle cell lymphoma | Mantle zone | Small | CD5+, CD23-, CD43+, Cyclin D1+[14] | Translocations ? | Clinical ? | Other ? |
| Marginal zone lymphoma (MALT) | Marginal zone | Small | CD21+, CD11c+, CD5-, CD23-[14] | Translocations | Clinical | Other |
| Precursor lymphoblastic lymphoma/leukemia | Location ? | Small | CD10+, CD5-, TdT+, CD99+[14] | Translocations ? | Clinical ? | Other ? |
Medium and large cell lymphomas:
| Name | Location | Size of cells | IHC | Translocations | Clinical | Other |
|---|---|---|---|---|---|---|
| Burkitt's lymphoma | Follicle | Large cells | CD10, bcl-6 | t(8;14) (q24;q32) | Rapid growth | "Starry sky" |
| Diffuse large B cell lymphoma | Follicle (?) | Large 4-5X of lymphocyte | MIB-1 >40% | none/like follicular l. | Poor prognosis | Common among lymphomas |
| Name | Location | Size of cells | IHC | Translocations | Clinical | Other |
Population cell marker quantification
Two techniques:
- Flow cytometry.
- Laser scanning cytometry (LSC).
Common markers:
- CD3, CD4, CD8, CD5, CD7.
- CD19, CD20, FMC7.
- Kappa, lambda.
Normal:
- T-cells to B-cells usually 1:1.
- In reactive nodes T-cell predominate.
- Normal thymic tissue has cells that are positive for both CD4 and CD8.
- Kappa (k) and lambda (l) are not expressed by the same cell.
- Rule-of-thumb for normal k:l range is: <6:1 and 1:<3.[15]
- Lambda dominance is less common.
GS guidelines - non-malignant is:[16]
- CD19 ~= CD20
- CD5 = CD3
- CD2 > CD3 and CD5
- CD4 + CD8 ~= CD3
- CD7 = the smalest number of T-cell
Abnormal:
- CD4>CD8 predominance classically seen in:
- Sarcoidosis.
- Hodgkin's lymphoma.
- T cell lymphoma - loss of one of the T-cell markers (CD2, CD3, CD5 or CD7).
Sample report
B-Cell Associated Markers
- CD10.
- Germinal centre marker.
- +ve in: follicular l., Burkitt l., precursor lymphoblastic leukemia.
- CD19.
- B cell marker.
- Should be ~=CD20.
- CD20.
- B cell marker.
- Should be ~=CD20.
- CD23.
- +ve in CLL/SLL.
- FMC7
- B cell marker.
- Kappa+CD19/20+.
- B cell clonality.
- Lambda+CD19/20+
- B cell clonality.
T-Cell Associated Markers
- CD3.
- CD3 ~= CD4 + CD8.
- Usually: CD2 > CD3 > CD7.
- CD5.
- Usually: CD2 > CD5 > CD7.
- CD4.
- CD3 ~= CD4 + CD8.
- CD8.
- CD3 ~= CD4 + CD8.
- CD7.
- Usually least prevalent T cell marker; < CD2, < CD3, < CD5.
- CD2.
- Usually most prevalent T cell marker; > CD3, > CD5, > CD7.
NK-Cell Associated Markers
- CD56.
- CD16.
Miscellaneous Markers
- CD11c.
- CD14.
See also
References
- ↑ DB. 5 August 2010.
- ↑ http://emedicine.medscape.com/article/1357846-overview
- ↑ http://emedicine.medscape.com/article/1357846-diagnosis
- ↑ 4.0 4.1 Alanen A, Pira U, Lassila O, Roth J, Franklin RM (March 1985). "Mott cells are plasma cells defective in immunoglobulin secretion". Eur. J. Immunol. 15 (3): 235–42. PMID 3979421.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 567. ISBN 978-0781765275.
- ↑ PMID: 9499174
- ↑ 7.0 7.1 7.2 Vitolo U, Ferreri AJ, Montoto S (June 2008). "Follicular lymphomas". Crit. Rev. Oncol. Hematol. 66 (3): 248–61. doi:10.1016/j.critrevonc.2008.01.014. PMID 18359244.
- ↑ Bacon CM, Du MQ, Dogan A (April 2007). "Mucosa-associated lymphoid tissue (MALT) lymphoma: a practical guide for pathologists". J. Clin. Pathol. 60 (4): 361–72. doi:10.1136/jcp.2005.031146. PMC 2001121. PMID 16950858. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2001121/.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 676 (???). ISBN 0-7216-0187-1.
- ↑ 10.0 10.1 10.2 10.3 10.4 10.5 Bellan C, Lazzi S, De Falco G, Nyongo A, Giordano A, Leoncini L (March 2003). "Burkitt's lymphoma: new insights into molecular pathogenesis". J. Clin. Pathol. 56 (3): 188–92. PMC 1769902. PMID 12610094. http://jcp.bmj.com/cgi/pmidlookup?view=long&pmid=12610094.
- ↑ URL: http://www.thefreelibrary.com/Dutcher+bodies+in+chronic+synovitis-a083551789. Accessed on: 4 August 2010.
- ↑ AML. Harrison's 16th Ed.
- ↑ AG. 8 July, 2009.
- ↑ 14.0 14.1 14.2 14.3 Lester, Susan Carole (2005). Manual of Surgical Pathology (2nd ed.). Saunders. pp. 95. ISBN 978-0443066450.
- ↑ SB. March 10, 2010.
- ↑ GS. LSC Procedure. March 11, 2010.