Difference between revisions of "Hodgkin lymphoma"
m (→Microscopic) |
m (fill in BCL6 and MUM1 in comparison table) |
||
| (26 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
'''Hodgkin [[lymphoma]]''', abbreviated '''HL''', is a malignancy that | {{ Infobox diagnosis | ||
| Name = Classical Hodgkin lymphoma | |||
| Image = Hodgkin_lymphoma_cytology_large.jpg | |||
| Width = | |||
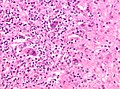
| Caption = HL mixed cellularity - cytology. | |||
| Micro = Reed-Sternberg cell (large binucleated cell (>= 45 micrometres), +/-multinucleated, +/-horseshoe-like shape, [[macronucleolus]] - approximately the size of a RBC (~8 micrometers)), well-defined cell border, abundant cytoplasm. | |||
| Subtypes = nodular sclerosis CHL, mixed cellularity CHL, lymphocyte-rich CHL, lymphocyte-depleted CHL | |||
| LMDDx = [[diffuse large B cell lymphoma]] (esp. ''T-cell/histiocytic-rich LBCL''), [[anaplastic large cell lymphoma]], | |||
B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma, nodular lymphocyte-predominant Hodgkin lymphoma | |||
| Stains = | |||
| IHC = CD30 Reed-Sternberg cells (RSCs) +ve ~98%, CD15 Reed-Sternberg cells +ve ~80% (also stains neutrophils), CD45 ''often negative'' in RSCs, CD20 -ve/+ve, PAX5 +ve | |||
| EM = | |||
| Molecular = | |||
| IF = | |||
| Gross = | |||
| Grossing = | |||
| Site = usu. [[lymph node]] - classically in the neck | |||
| Assdx = | |||
| Syndromes = | |||
| Clinicalhx = young adults, older adults (bimodal distribution) | |||
| Signs = lymphadenopathy - usu. neck, +/-[[B symptoms]] (fever, night sweats, weight loss) | |||
| Symptoms = | |||
| Prevalence = common | |||
| Bloodwork = | |||
| Rads = | |||
| Endoscopy = | |||
| Prognosis = usu. good, dependent on stage | |||
| Other = | |||
| ClinDDx = | |||
}} | |||
'''Hodgkin [[lymphoma]]''', abbreviated '''HL''', is a haematological [[malignancy]]. If not otherwise specified, Hodgkin lymphoma generally refers to classical Hodgkin lymphoma (CHL) rather than [[nodular lymphocyte-predominant Hodgkin lymphoma]] (NLPHL). The latter accounts for only about 5% of the loose label of Hodgkin lymphoma<ref name=Ref_WMSP567/> and shows a sufficiently different biology and immunophenotype that is essentially a different disease (see [[nodular lymphocyte-predominant Hodgkin lymphoma|main article on NLPHL]]). The common feature is large atypical cells: Hodgkin/Reed-Sternberg cells in the case of classical Hodgkin lymphoma and "popcorn"/lymphohistiocytic/L&H cells in NLPHL. However, at least in typical cases, there are morphological and immunophenotypic differences. | |||
Classical Hodgkin lymphoma has a bi-modal distribution, afflicting young adults and with a further peak in incidence in middle-age. Fortunately, it usually has a good prognosis. | |||
==Clinical== | Pathologists say "... it is both the easiest and hardest diagnosis to make." The reason for this is: the diagnosis depends on finding Reed-Sternberg cells (or Popcorn cells); if they are obvious the diagnosis is easy... if you can't find 'em and an alternative diagnosis is not apparent -- you wonder whether you're missing them. | ||
==General== | |||
===Clinical=== | |||
Symptoms:<ref name=Ref_WMSP567>{{Ref WMSP|567}}</ref> | Symptoms:<ref name=Ref_WMSP567>{{Ref WMSP|567}}</ref> | ||
*"B symptoms":<ref>URL: [http://lymphoma.about.com/od/symptoms/f/bsymptoms.htm http://lymphoma.about.com/od/symptoms/f/bsymptoms.htm]. Accessed on: 11 August 2010.</ref> | *"[[B symptoms]]" - all required:<ref>URL: [http://lymphoma.about.com/od/symptoms/f/bsymptoms.htm http://lymphoma.about.com/od/symptoms/f/bsymptoms.htm]. Accessed on: 11 August 2010.</ref> weight loss, night sweats and fever. | ||
*Infections | *Infections due to immune dysfunction. | ||
Diagnosis: | Diagnosis: | ||
| Line 12: | Line 45: | ||
Prognosis: | Prognosis: | ||
* | *Usually good. | ||
*Unlike non-Hodgkin lymphomas, it spreads in a predictable pattern; thus, staging plays an important role in determining the therapy.<ref>{{Ref PCPBoD8|315}}</ref> | *Unlike non-Hodgkin lymphomas, it spreads in a predictable pattern; thus, staging plays an important role in determining the therapy.<ref name=PCPBoD8_315>{{Ref PCPBoD8|315}}</ref> | ||
*Clinically classified into early favourable, early unfavourable and late/advanced disease. | |||
* | |||
===Classic HL sub-types=== | |||
====Subtypes of classic HL==== | ====Subtypes of classic HL==== | ||
There are four CHL subtypes:<ref name=Ref_WMSP567/> | There are four CHL subtypes:<ref name=Ref_WMSP567/> | ||
| Line 66: | Line 66: | ||
*The subtypes prevalence is in reverse alphabetical order. | *The subtypes prevalence is in reverse alphabetical order. | ||
=== | ==Gross== | ||
Location: | |||
*'' | *Almost always arises from a [[lymph node]] - classically in the neck, but may be in the axilla and mediastinum | ||
* | *Spleen may be involved | ||
** | *Bone marrow involvement is unusual (~5% of cases, higher in HIV-associated cases), so bone marrow assessment is usually not performed | ||
** | *''Extranodal Hodgkin lymphoma'' is (case report) rare.<ref name=pmid11100066>{{Cite journal | last1 = Vadmal | first1 = MS. | last2 = LaValle | first2 = GP. | last3 = DeYoung | first3 = BR. | last4 = Frankel | first4 = WL. | last5 = Marsh | first5 = WL. | title = Primary localized extranodal hodgkin disease of the transverse colon. | journal = Arch Pathol Lab Med | volume = 124 | issue = 12 | pages = 1824-7 | month = Dec | year = 2000 | doi = 10.1043/0003-9985(2000)1241824:PLEHDO2.0.CO;2 | PMID = 11100066 }}</ref> | ||
* | |||
==Microscopic== | |||
Defined by ''Reed-Sternberg cells'' (RSCs). Morphologically similar mononuclear cells are known as Hodgkin cells. RSCs are: | |||
*Large binucleated cell (>= 45 micrometres).<ref name=Ref_PCPBoD8_329>{{Ref PCPBoD8|329}}</ref> | |||
**May be multinucleated. | |||
**May have a horseshoe-like shape. | |||
*[[Macronucleolus]] - approximately the size of a RBC (~8 micrometers). | |||
*Well-defined cell border. | |||
*Abundant cytoplasm. | |||
RSC may show peri-cellular clearing, making the cells appear within a space. These are called lacunar cells (as they are in a "lake"). Apoptotic RSC may show pyknotic nuclei and scant eosinophilic cytoplasm and are sometimes known as "mummified" cells. | |||
Images ( | ===Images (classic HL)=== | ||
<gallery> | |||
Image:CHL mummified cell x40.jpg | "Mummified" RSC. (WC) | |||
Image:CHL lacunar cell x40.jpg | "Lacunar cell". (WC) | |||
Image:16S14098 cHL multinucleate HRS cell x40c.jpg | Multinucleate RSC. (WC) | |||
Image:Hodgkin_lymphoma_cytology_large.jpg | HL mixed cellularity - cytology. (WC) | |||
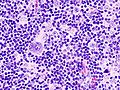
Image:Hodgkin_lymphoma_cytology_small.jpg | HL mixed cellularity - cytology. (WC) | |||
Image:Hodgkin_lymphoma_%281%29_mixed_cellulary_type.jpg | HL mixed cellularity. (WC) | |||
</gallery> | |||
===DDx both CHL & NLPHL=== | ===DDx both CHL & NLPHL=== | ||
*CHL/NLPHL. | *CHL/NLPHL. | ||
*[[Diffuse large B cell lymphoma]] (DLBCL). | *[[Diffuse large B cell lymphoma]] (DLBCL), esp. ''T-cell/histiocytic-rich LBCL''. | ||
*[[Anaplastic large cell lymphoma]] (ALCL). | *[[Anaplastic large cell lymphoma]] (ALCL). | ||
*B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma.<ref name=pmid22222636>{{Cite journal | last1 = Gualco | first1 = G. | last2 = Natkunam | first2 = Y. | last3 = Bacchi | first3 = CE. | title = The spectrum of B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma: a description of 10 cases. | journal = Mod Pathol | volume = | issue = | pages = | month = Jan | year = 2012 | doi = 10.1038/modpathol.2011.200 | PMID = 22222636 | URL = http://www.nature.com/modpathol/journal/vaop/ncurrent/full/modpathol2011200a.html }}</ref> (typically in cases of numerous large atypical cells where the morphology and immunophenotype do not neatly fit into either DLBCL or CHL). | |||
==IHC== | ==IHC== | ||
Abbreviated panel:<ref name=Ref_WMSP568>{{Ref_WMSP|568}}</ref> | Abbreviated panel:<ref name=Ref_WMSP568>{{Ref_WMSP|568}}</ref> | ||
*CD30 Reed-Sternberg cells (RSCs) +ve ~98% | *CD30 Reed-Sternberg cells (RSCs) +ve ~98% (beware of mis-interpreting CD30+ activated lymphoid cells) | ||
*CD15 Reed-Sternberg cells +ve ~80%, stains neutrophils. | *CD15 Reed-Sternberg cells +ve ~80%, stains neutrophils. | ||
*Both CD30 and CD15 are classically positive in a membranous and Golgi pattern | |||
*MUM1 +ve | |||
*CD45 '''often negative''' in RSCs. | *CD45 '''often negative''' in RSCs. | ||
*CD20 may stain RSCs. | *CD20 may stain RSCs (usually negative, but can be weak). | ||
*PAX5 +ve | *PAX5 +ve, though said to be weaker than background normal B-cells<ref name=Ref_APBR683>{{Ref APBR|683}}</ref> | ||
Additional - for completeness: | Additional - for completeness: | ||
*CD3 (T lymphocytes) | *CD3 (T lymphocytes) - negative in RSCs | ||
*OCT2/BOB1 negative (co-transcription factors for immunoglobulin production, one or the other is usually negative) | |||
*40% are EBV positive. | |||
NLPHL IHC '''differs''' from the classical HL:<ref name=Ref_APBR683>{{Ref APBR|683}}</ref> | NLPHL IHC '''differs''' from the classical HL:<ref name=Ref_APBR683>{{Ref APBR|683}}</ref> | ||
| Line 99: | Line 120: | ||
*CD10 +ve. | *CD10 +ve. | ||
*Bcl-6 +ve. | *Bcl-6 +ve. | ||
*EMA +ve | *[[EMA]] +ve (40-50%) | ||
*CD30 -ve | *CD30 -ve | ||
*CD15 -ve. | *CD15 -ve. | ||
=== | ===A panel=== | ||
{| class="wikitable" | {| class="wikitable" | ||
|Antibody || NLPHL || CHL | |Antibody || NLPHL || CHL | ||
| Line 111: | Line 132: | ||
|CD20 || +ve || -ve | |CD20 || +ve || -ve | ||
|- | |- | ||
|BCL6 || || | |BCL6 || +ve || -ve | ||
|- | |- | ||
|MUM1<ref>URL: [http://www.ncbi.nlm.nih.gov/omim/601900 http://www.ncbi.nlm.nih.gov/omim/601900]. Accessed on: 10 August 2010.</ref> || -ve || | |MUM1<ref>URL: [http://www.ncbi.nlm.nih.gov/omim/601900 http://www.ncbi.nlm.nih.gov/omim/601900]. Accessed on: 10 August 2010.</ref> || -ve || +ve | ||
|- | |- | ||
|CD30 || -ve || +ve (most sensitive). | |CD30 || -ve || +ve (most sensitive). | ||
| Line 121: | Line 142: | ||
|CD21 || networks present || no networks | |CD21 || networks present || no networks | ||
|- | |- | ||
|CD23 | |[[CD23]] || networks present || no networks | ||
|- | |- | ||
|OCT-2 || +ve || -ve | |OCT-2 || +ve || -ve | ||
| Line 137: | Line 158: | ||
|4 unstained || || | |4 unstained || || | ||
|} | |} | ||
==Sign out== | |||
===Suggestive FNA=== | |||
<pre> | |||
Lymph Node, Right Neck, FNA: | |||
- Large binucleated and multinucleated cells with macronucleoli in | |||
a background of abundant lymphocytes, histiocytes, rare eosinophils. | |||
Comment: | |||
A cell block is not available for further work-up. The findings raise the possibility of Hodgkin's lymphoma. | |||
A further biopsy is required for the diagnosis. | |||
</pre> | |||
==See also== | ==See also== | ||
Latest revision as of 22:01, 4 December 2018
| Classical Hodgkin lymphoma | |
|---|---|
| Diagnosis in short | |
|
Template:Px HL mixed cellularity - cytology. | |
|
| |
| LM | Reed-Sternberg cell (large binucleated cell (>= 45 micrometres), +/-multinucleated, +/-horseshoe-like shape, macronucleolus - approximately the size of a RBC (~8 micrometers)), well-defined cell border, abundant cytoplasm. |
| Subtypes | nodular sclerosis CHL, mixed cellularity CHL, lymphocyte-rich CHL, lymphocyte-depleted CHL |
| LM DDx |
diffuse large B cell lymphoma (esp. T-cell/histiocytic-rich LBCL), anaplastic large cell lymphoma, B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma, nodular lymphocyte-predominant Hodgkin lymphoma |
| IHC | CD30 Reed-Sternberg cells (RSCs) +ve ~98%, CD15 Reed-Sternberg cells +ve ~80% (also stains neutrophils), CD45 often negative in RSCs, CD20 -ve/+ve, PAX5 +ve |
| Site | usu. lymph node - classically in the neck |
|
| |
| Clinical history | young adults, older adults (bimodal distribution) |
| Signs | lymphadenopathy - usu. neck, +/-B symptoms (fever, night sweats, weight loss) |
| Prevalence | common |
| Prognosis | usu. good, dependent on stage |
Hodgkin lymphoma, abbreviated HL, is a haematological malignancy. If not otherwise specified, Hodgkin lymphoma generally refers to classical Hodgkin lymphoma (CHL) rather than nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL). The latter accounts for only about 5% of the loose label of Hodgkin lymphoma[1] and shows a sufficiently different biology and immunophenotype that is essentially a different disease (see main article on NLPHL). The common feature is large atypical cells: Hodgkin/Reed-Sternberg cells in the case of classical Hodgkin lymphoma and "popcorn"/lymphohistiocytic/L&H cells in NLPHL. However, at least in typical cases, there are morphological and immunophenotypic differences.
Classical Hodgkin lymphoma has a bi-modal distribution, afflicting young adults and with a further peak in incidence in middle-age. Fortunately, it usually has a good prognosis.
Pathologists say "... it is both the easiest and hardest diagnosis to make." The reason for this is: the diagnosis depends on finding Reed-Sternberg cells (or Popcorn cells); if they are obvious the diagnosis is easy... if you can't find 'em and an alternative diagnosis is not apparent -- you wonder whether you're missing them.
General
Clinical
Symptoms:[1]
- "B symptoms" - all required:[2] weight loss, night sweats and fever.
- Infections due to immune dysfunction.
Diagnosis:
- HL cannot be diagnosed with standard flow cytometry (FC) - but has been diagnosed with specialized FC.[3]
Prognosis:
- Usually good.
- Unlike non-Hodgkin lymphomas, it spreads in a predictable pattern; thus, staging plays an important role in determining the therapy.[4]
- Clinically classified into early favourable, early unfavourable and late/advanced disease.
Classic HL sub-types
Subtypes of classic HL
There are four CHL subtypes:[1]
- Nodular sclerosis CHL - ~70% of CHL.
- Mixed cellular background - T cell, plasma cells, eosinophils, neutrophils and histiocytes.
- Nodular sclerosing fibrosis - thick strands fibrosis.
- Mixed cellularity CHL - ~20-25% of CHL.
- Lymphocyte-rich CHL - rare.
- T lymphocytes only (no mix of cells).
- Lymphocyte-depleted CHL - rare.
- May be associated with HIV infection.[5]
Memory device:
- The subtypes prevalence is in reverse alphabetical order.
Gross
Location:
- Almost always arises from a lymph node - classically in the neck, but may be in the axilla and mediastinum
- Spleen may be involved
- Bone marrow involvement is unusual (~5% of cases, higher in HIV-associated cases), so bone marrow assessment is usually not performed
- Extranodal Hodgkin lymphoma is (case report) rare.[6]
Microscopic
Defined by Reed-Sternberg cells (RSCs). Morphologically similar mononuclear cells are known as Hodgkin cells. RSCs are:
- Large binucleated cell (>= 45 micrometres).[7]
- May be multinucleated.
- May have a horseshoe-like shape.
- Macronucleolus - approximately the size of a RBC (~8 micrometers).
- Well-defined cell border.
- Abundant cytoplasm.
RSC may show peri-cellular clearing, making the cells appear within a space. These are called lacunar cells (as they are in a "lake"). Apoptotic RSC may show pyknotic nuclei and scant eosinophilic cytoplasm and are sometimes known as "mummified" cells.
Images (classic HL)

"Mummified" RSC. (WC)

"Lacunar cell". (WC)
Multinucleate RSC. (WC)

HL mixed cellularity - cytology. (WC)

HL mixed cellularity - cytology. (WC)
HL mixed cellularity. (WC)





_mixed_cellulary_type.jpg)
DDx both CHL & NLPHL
- CHL/NLPHL.
- Diffuse large B cell lymphoma (DLBCL), esp. T-cell/histiocytic-rich LBCL.
- Anaplastic large cell lymphoma (ALCL).
- B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma.[8] (typically in cases of numerous large atypical cells where the morphology and immunophenotype do not neatly fit into either DLBCL or CHL).
IHC
Abbreviated panel:[9]
- CD30 Reed-Sternberg cells (RSCs) +ve ~98% (beware of mis-interpreting CD30+ activated lymphoid cells)
- CD15 Reed-Sternberg cells +ve ~80%, stains neutrophils.
- Both CD30 and CD15 are classically positive in a membranous and Golgi pattern
- MUM1 +ve
- CD45 often negative in RSCs.
- CD20 may stain RSCs (usually negative, but can be weak).
- PAX5 +ve, though said to be weaker than background normal B-cells[10]
Additional - for completeness:
- CD3 (T lymphocytes) - negative in RSCs
- OCT2/BOB1 negative (co-transcription factors for immunoglobulin production, one or the other is usually negative)
- 40% are EBV positive.
NLPHL IHC differs from the classical HL:[10]
- LCA +ve.
- CD20 +ve.
- CD10 +ve.
- Bcl-6 +ve.
- EMA +ve (40-50%)
- CD30 -ve
- CD15 -ve.
A panel
| Antibody | NLPHL | CHL |
| CD45 | +ve | -ve |
| CD20 | +ve | -ve |
| BCL6 | +ve | -ve |
| MUM1[11] | -ve | +ve |
| CD30 | -ve | +ve (most sensitive). |
| CD15 | -ve | +ve |
| CD21 | networks present | no networks |
| CD23 | networks present | no networks |
| OCT-2 | +ve | -ve |
| PAX5 | +ve | +ve (proves B cell linage) |
| CD3 | usu. < benign B cell | usu. > benign B cell component |
| CD57 | rosettes around malign. cells | - |
| EBER | -ve | +ve/-ve |
| EMA | +ve/-ve | -ve |
| 4 unstained |
Sign out
Suggestive FNA
Lymph Node, Right Neck, FNA: - Large binucleated and multinucleated cells with macronucleoli in a background of abundant lymphocytes, histiocytes, rare eosinophils. Comment: A cell block is not available for further work-up. The findings raise the possibility of Hodgkin's lymphoma. A further biopsy is required for the diagnosis.
See also
References
- ↑ 1.0 1.1 1.2 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 567. ISBN 978-0781765275.
- ↑ URL: http://lymphoma.about.com/od/symptoms/f/bsymptoms.htm. Accessed on: 11 August 2010.
- ↑ Fromm JR, Thomas A, Wood BL (March 2009). "Flow cytometry can diagnose classical hodgkin lymphoma in lymph nodes with high sensitivity and specificity". Am. J. Clin. Pathol. 131 (3): 322–32. doi:10.1309/AJCPW3UN9DYLDSPB. PMID 19228638.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 315. ISBN 978-1416054542.
- ↑ 5.0 5.1 Sissolak G, Sissolak D, Jacobs P (April 2010). "Human immunodeficiency and Hodgkin lymphoma". Transfus. Apher. Sci. 42 (2): 131–9. doi:10.1016/j.transci.2010.01.008. PMID 20138008.
- ↑ Vadmal, MS.; LaValle, GP.; DeYoung, BR.; Frankel, WL.; Marsh, WL. (Dec 2000). "Primary localized extranodal hodgkin disease of the transverse colon.". Arch Pathol Lab Med 124 (12): 1824-7. doi:10.1043/0003-9985(2000)1241824:PLEHDO2.0.CO;2. PMID 11100066.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 329. ISBN 978-1416054542.
- ↑ Gualco, G.; Natkunam, Y.; Bacchi, CE. (Jan 2012). "The spectrum of B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma: a description of 10 cases.". Mod Pathol. doi:10.1038/modpathol.2011.200. PMID 22222636.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 568. ISBN 978-0781765275.
- ↑ 10.0 10.1 Lefkowitch, Jay H. (2006). Anatomic Pathology Board Review (1st ed.). Saunders. pp. 683. ISBN 978-1416025887.
- ↑ URL: http://www.ncbi.nlm.nih.gov/omim/601900. Accessed on: 10 August 2010.