Difference between revisions of "Primary biliary cholangitis"
m (touch) |
m |
||
| (10 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
{{ Infobox diagnosis | {{ Infobox diagnosis | ||
| Name = {{PAGENAME}} | | Name = {{PAGENAME}} | ||
| Image = | | Image = Primary_biliary_cirrhosis_intermed_mag.jpg | ||
| Width = | | Width = | ||
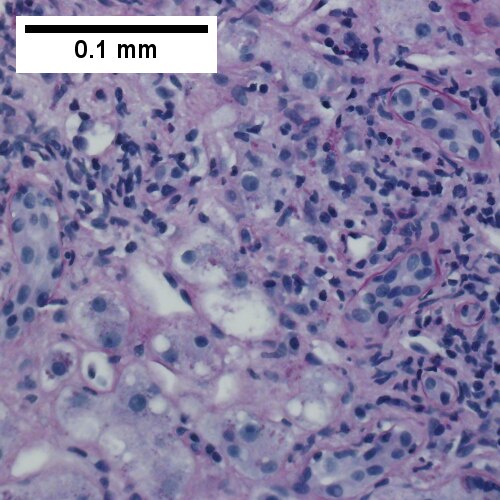
| Caption = Primary biliary | | Caption = Primary biliary cholangitis. [[H&E stain]]. | ||
| Synonyms = primary biliary cirrhosis (obsolete term) | |||
| Micro = "florid duct lesion": intraepithelial lymphocytes - in bile duct, bile duct epithelial cells with eosinophilic cytoplasm; plasma cells; +/-[[granulomas]] (close to bile duct); +/-"garland" cirrhosis -- has irregular border | | Micro = "florid duct lesion": intraepithelial lymphocytes - in bile duct, bile duct epithelial cells with eosinophilic cytoplasm; plasma cells; +/-[[granulomas]] (close to bile duct); +/-"garland" cirrhosis -- has irregular border | ||
| Subtypes = | | Subtypes = | ||
| Line 28: | Line 29: | ||
| ClinDDx = | | ClinDDx = | ||
}} | }} | ||
'''Primary biliary | '''Primary biliary cholangitis''', abbreviated '''PBC''', is a rare [[medical liver disease]]. | ||
It was previously known as ''primary ciliary cirrhosis''.<ref name=pmid26416194>{{cite journal |authors=Beuers U, Gershwin ME, Gish RG, Invernizzi P, Jones DE, Lindor K, Ma X, Mackay IR, Parés A, Tanaka A, Vierling JM, Poupon R |title=Changing Nomenclature for PBC: From 'Cirrhosis' to 'Cholangitis' |journal=Am J Gastroenterol |volume=110 |issue=11 |pages=1536–8 |date=November 2015 |pmid=26416194 |pmc=4679751 |doi=10.1038/ajg.2015.312 |url=}}</ref> | |||
==General== | ==General== | ||
| Line 81: | Line 84: | ||
Image:Primary_biliary_cirrhosis_low_mag.jpg | PBC - low mag. (WC) | Image:Primary_biliary_cirrhosis_low_mag.jpg | PBC - low mag. (WC) | ||
Image:Primary_biliary_cirrhosis_intermed_mag.jpg | PBC - intermed. mag. (WC) | Image:Primary_biliary_cirrhosis_intermed_mag.jpg | PBC - intermed. mag. (WC) | ||
Image:Primary_biliary_cirrhosis_intermed_mag_2.jpg | PBC - intermed. mag. (WC) | |||
</gallery> | </gallery> | ||
www: | www: | ||
*[http://www.gidesigns.net/images/MC-copper-flower-garland-L.jpg Garland - wreath of flowers (gidesigns.net)]. | *[http://www.gidesigns.net/images/MC-copper-flower-garland-L.jpg Garland - wreath of flowers (gidesigns.net)]. | ||
{| | |||
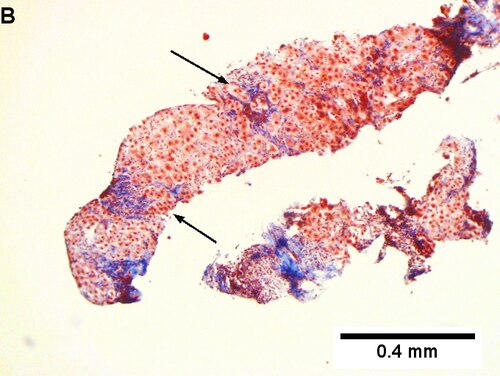
[[File:1 PBC 4 680x512px.tif|Inflamed triads [arrows] amid undisturbed hepatocytes (Row 1 Left 40X).]] | |||
[[File:2 PBC 4 680x512px.tif|Granuloma in portal triad (Row 1 Right 400X).]] | |||
<br> | |||
[[File:3 PBC 4 680x512px.tif|Florid duct lesion (Row 2 Left 400X).]] | |||
[[File:4 PBC 4 680x512px.tif|Triad missing interlobular bile duct (Row 2 Right 400X).]] | |||
|} | |||
Primary biliary cirrhosis. Inflamed triads [arrows] amid undisturbed hepatocytes (Row 1 Left 40X). Granuloma in portal triad (Row 1 Right 400X). Florid duct lesion (Row 2 Left 400X). Triad missing interlobular bile duct (Row 2 Right 400X). | |||
{| | |||
[[File:1 PBC 3 680x512px.tif| Ill defined triads, inflamed lobule (40X).]] | |||
[[File:2 PBC 3 680x512px.tif| Triad without a bile duct. Macrophages & occasional lymphocytes without epithelioid cells needed for granuloma and space where bile duct likely once was [cyan arrowhead] (400X).]] | |||
<br> | |||
[[File:3 PBC 3 680x512px.tif| PAS without diastase shows triad lacking bile duct and piecemeal necrosis (200X).]] | |||
[[File:4 PBC 3 680x512px.tif| PAS with diastase shows bile duct/proliferating bile ductules with epithelial injury and hepatocytes with ballooning degeneration (400X).]] | |||
<br> | |||
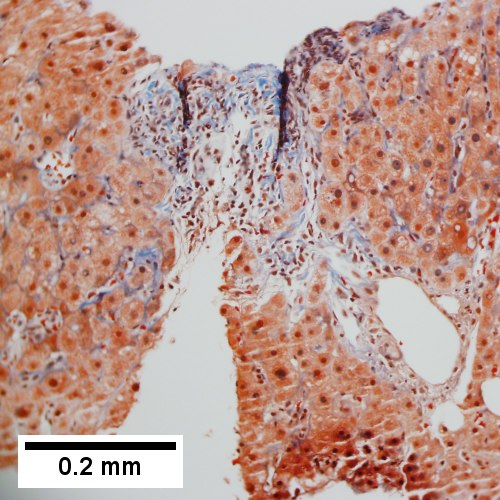
[[File:5 PBC 3 680x512px.tif| Trichrome shows space of Disse collagenization and periportal fibrosis without definite bridging (100X)..]] | |||
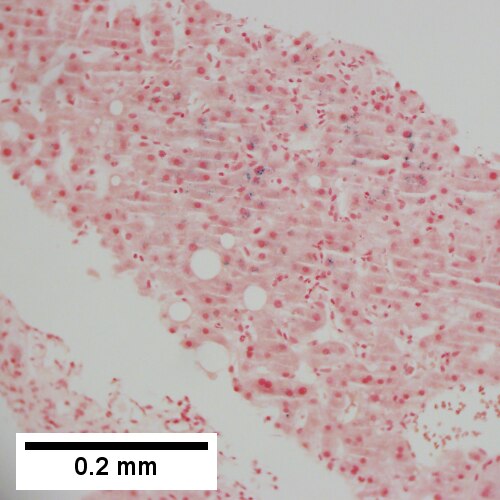
[[File:6 PBC 3 680x512px.tif| Iron stain shows isolated focus of hepatocytes with cytoplasmic blue granules (200X)]] | |||
|} | |||
Primary biliary cirrhosis. AMA positive. Viral serology/ANA negative. No definite granulomas. Ill defined triads, inflamed lobule (Row 1 Left 40X). Triad without a bile duct. Macrophages & occasional lymphocytes without epithelioid cells needed for granuloma and space where bile duct likely once was [cyan arrowhead] (Row 1 Right 400X). PAS without diastase shows triad lacking bile duct and piecemeal necrosis (Row 2 Left 200X). PAS with diastase shows bile duct/proliferating bile ductules with epithelial injury and hepatocytes with ballooning degeneration (Row 2 Right 400X). Trichrome shows space of Disse collagenization and periportal fibrosis without definite bridging (Row 3 Left 100X). Iron stain shows isolated focus of hepatocytes with cytoplasmic blue granules (Row 3 Right 200X). | |||
{| | |||
[[File:1 PBC 2 680x512px.tif|Two inflamed triads accompany acini with mild steatosis (20X).]] | |||
[[File:2 PBC 2 680x512px.tif|A triad bears a poorly formed granuloma [yellow arrowhead]. A bile duct is also seen [red arrowhead] (200X).]] | |||
<br> | |||
[[File:3 PBC 2 680x512px.tif|A triad lacks a bile duct (200X).]] | |||
[[File:4 PBC 2 680x512px.tif|Trichrome of the same triad shows portal fibrosis (200X).]] | |||
|} | |||
Primary biliary cirrhosis. Two inflamed triads accompany acini with mild steatosis (Row 1 Left 20X). A triad bears a poorly formed granuloma [yellow arrowhead]. A bile duct is also seen [red arrowhead] (Row 1 Right 200X). A triad lacks a bile duct (Row 2 Left 200X). Trichrome of the same triad shows portal fibrosis (Row 2 Right 200X). | |||
{| | |||
[[File:1 PBC - 1 - 40X 680x512px.tif|Acini & lobules distorted by inflammation]] | |||
[[File:2 PBC - 1 - 200X 680x512px.tif|Loose granuloma in triad without duct]] | |||
<br> | |||
[[File:3 PBC - 1 - 200X 680x512px.tif|Well-formed granuloma]] | |||
[[File:4 PBC - 1 -200X 680x512px.tif|Piecemeal necrosis, PAS without diastase]] | |||
<br> | |||
[[File:5 PBC - 1 -400X 680x512px.tif|Damaged bile duct, PAS with diastase]] | |||
[[File:6 PBC - 1 -200X 680x512px.tif|Bridging fibrosis, trichrome]] | |||
|} | |||
Primary biliary cirrhosis with bridging fibrosis. Acini & lobules distorted by inflammation (Row 1 Left 40X) Loose granuloma in triad without duct (Row 1 Right 200X) Well-formed granuloma (Row 2 Left 200X) Piecemeal necrosis, PAS without diastase (Row 2 Right 200X) Damaged bile duct, PAS with diastase (Row 3 Left 400X) Bridging fibrosis, trichrome (Row 3 Right,200X) | |||
{| | |||
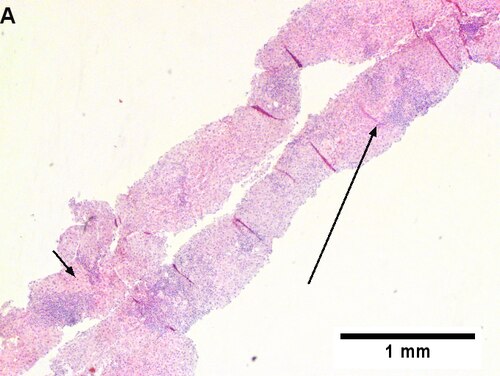
[[File:1 PBC 5 680x512px.tif|Stage 4 PBC.]] | |||
[[File:2 PBC 5 680x512px.tif| Stage 4 PBC.]] | |||
<br> | |||
[[File:3 PBC 5 680x512px.tif| Stage 4 PBC.]] | |||
[[File:4 PBC 5 680x512px.tif| Stage 4 PBC.]] | |||
<br> | |||
[[File:5 PBC 5 680x512px.tif| Stage 4 PBC.]] | |||
[[File:6 PBC 5 680x512px.tif| Stage 4 PBC.]] | |||
|} | |||
Primary biliary cirrhosis with Metavir stage 4 fibrosis (extensive fibrosis/cirrhosis). The patient was AMA positive and ANA negative. A. Inflamed tracts and bridges are intensely inflamed, with odd appearing edges of hepatocytes (arrows), suggestive of a jig saw pattern [40x]. B. Trichrome shows thin fibrous bands bounding regenerative isles (arrows) [Trichrome, 100X]. C. Reticulin shows two cell thick cords and cords lacking orientation, documenting regeneration; black lines about single cells document piecemeal necrosis [100X]. D. Lymphocytes, plasma cells, and macrophages, show piecemeal necrosis, surrounding hepatocytes (cyan arrows), as well as spreading into the lobule (green arrows), with aggregates reflecting spotty necrosis (black arrow). [400X]. E. PAS with diastase highlights a proliferated bile ductule (arrows) with epithelial damage [400X]. F. PAS with diastase shows an arteriole (green arrow) at great distance from an isolated bile ductule at the periphery of the triad (cyan arrow), consistent with loss of bile duct; neutrophils (black arrows) do not prove ascending cholangitis [400X]. | |||
===Staging PBC=== | ===Staging PBC=== | ||
Latest revision as of 22:29, 9 October 2021
| Primary biliary cholangitis | |
|---|---|
| Diagnosis in short | |
 Primary biliary cholangitis. H&E stain. | |
|
| |
| Synonyms | primary biliary cirrhosis (obsolete term) |
|
| |
| LM | "florid duct lesion": intraepithelial lymphocytes - in bile duct, bile duct epithelial cells with eosinophilic cytoplasm; plasma cells; +/-granulomas (close to bile duct); +/-"garland" cirrhosis -- has irregular border |
| LM DDx | sarcoidosis, primary sclerosing cholangitis, viral hepatitis, autoimmune hepatitis, drug-induced liver disease, Hodgkin's lymphoma |
| Site | liver - see medical liver diseases |
|
| |
| Associated Dx | other autoimmune conditions, e.g. celiac disease, Sjögren syndrome |
| Clinical history | woman, middle age |
| Symptoms | pruritis |
| Blood work | AMA +ve |
Primary biliary cholangitis, abbreviated PBC, is a rare medical liver disease.
It was previously known as primary ciliary cirrhosis.[1]
General
Epidemiology:
- Female>male (~9:1).[2]
- Usually middle age.
- Associated with other autoimmune conditions (Sjögren syndrome, progressive systemic sclerosis, celiac disease).
Etiology:
- Autoimmune.
Serology:
- AMA +ve.[3]
Classic presentation:
- Pruritis.
Pathophysiology:
- Septal bile duct attacked.
Treatment:
- Ursodeoxycholic acid.
- May be indication for transplant.
Microscopic
Features:
- "Florid duct lesion":[4]
- Intraepithelial lymphocytes - in bile duct - key feature.
- Bile duct epithelial cells with eosinophilic cytoplasm.[5]
- Plasma cells.
- Granulomas - close to bile duct.
- Seen in classic presentation -- often not present or poorly formed.
- Focal damage (may be missed on biopsy -- due to sampling).
- "Garland" cirrhosis -- has irregular border (unlike in EtOH).
- Garland originally "wreath of flowers" (in French).[6]
Notes:
- PAS stain useful for examining basement membrane... which is lost in PBC.
- Lobular inflammation should be minimal.
- May cause cholestatic picture.[7]
DDx:[8]
- Sarcoidosis (if granulomas present).
- Primary sclerosing cholangitis.
- Viral hepatitis.
- Autoimmune hepatitis.
- Drug-induced liver disease.
- Hodgkin's lymphoma.[9]
Images

PBC - low mag. (WC)
PBC - intermed. mag. (WC)
- Primary biliary cirrhosis intermed mag 2.jpg
PBC - intermed. mag. (WC)

www:
Inflamed triads [arrows] amid undisturbed hepatocytes (Row 1 Left 40X).Granuloma in portal triad (Row 1 Right 400X).{kind=link}
Florid duct lesion (Row 2 Left 400X).Triad missing interlobular bile duct (Row 2 Right 400X).
Primary biliary cirrhosis. Inflamed triads [arrows] amid undisturbed hepatocytes (Row 1 Left 40X). Granuloma in portal triad (Row 1 Right 400X). Florid duct lesion (Row 2 Left 400X). Triad missing interlobular bile duct (Row 2 Right 400X).
Ill defined triads, inflamed lobule (40X).Triad without a bile duct. Macrophages & occasional lymphocytes without epithelioid cells needed for granuloma and space where bile duct likely once was [cyan arrowhead] (400X).PAS without diastase shows triad lacking bile duct and piecemeal necrosis (200X).
Trichrome shows space of Disse collagenization and periportal fibrosis without definite bridging (100X)..
Primary biliary cirrhosis. AMA positive. Viral serology/ANA negative. No definite granulomas. Ill defined triads, inflamed lobule (Row 1 Left 40X). Triad without a bile duct. Macrophages & occasional lymphocytes without epithelioid cells needed for granuloma and space where bile duct likely once was [cyan arrowhead] (Row 1 Right 400X). PAS without diastase shows triad lacking bile duct and piecemeal necrosis (Row 2 Left 200X). PAS with diastase shows bile duct/proliferating bile ductules with epithelial injury and hepatocytes with ballooning degeneration (Row 2 Right 400X). Trichrome shows space of Disse collagenization and periportal fibrosis without definite bridging (Row 3 Left 100X). Iron stain shows isolated focus of hepatocytes with cytoplasmic blue granules (Row 3 Right 200X).
Two inflamed triads accompany acini with mild steatosis (20X).A triad bears a poorly formed granuloma [yellow arrowhead]. A bile duct is also seen [red arrowhead] (200X).A triad lacks a bile duct (200X).
Primary biliary cirrhosis. Two inflamed triads accompany acini with mild steatosis (Row 1 Left 20X). A triad bears a poorly formed granuloma [yellow arrowhead]. A bile duct is also seen [red arrowhead] (Row 1 Right 200X). A triad lacks a bile duct (Row 2 Left 200X). Trichrome of the same triad shows portal fibrosis (Row 2 Right 200X).
Acini & lobules distorted by inflammationLoose granuloma in triad without ductWell-formed granulomaPiecemeal necrosis, PAS without diastase
Damaged bile duct, PAS with diastaseBridging fibrosis, trichrome
Primary biliary cirrhosis with bridging fibrosis. Acini & lobules distorted by inflammation (Row 1 Left 40X) Loose granuloma in triad without duct (Row 1 Right 200X) Well-formed granuloma (Row 2 Left 200X) Piecemeal necrosis, PAS without diastase (Row 2 Right 200X) Damaged bile duct, PAS with diastase (Row 3 Left 400X) Bridging fibrosis, trichrome (Row 3 Right,200X)
Stage 4 PBC.Stage 4 PBC.
Stage 4 PBC.Stage 4 PBC.
Primary biliary cirrhosis with Metavir stage 4 fibrosis (extensive fibrosis/cirrhosis). The patient was AMA positive and ANA negative. A. Inflamed tracts and bridges are intensely inflamed, with odd appearing edges of hepatocytes (arrows), suggestive of a jig saw pattern [40x]. B. Trichrome shows thin fibrous bands bounding regenerative isles (arrows) [Trichrome, 100X]. C. Reticulin shows two cell thick cords and cords lacking orientation, documenting regeneration; black lines about single cells document piecemeal necrosis [100X]. D. Lymphocytes, plasma cells, and macrophages, show piecemeal necrosis, surrounding hepatocytes (cyan arrows), as well as spreading into the lobule (green arrows), with aggregates reflecting spotty necrosis (black arrow). [400X]. E. PAS with diastase highlights a proliferated bile ductule (arrows) with epithelial damage [400X]. F. PAS with diastase shows an arteriole (green arrow) at great distance from an isolated bile ductule at the periphery of the triad (cyan arrow), consistent with loss of bile duct; neutrophils (black arrows) do not prove ascending cholangitis [400X].
Staging PBC
PBC is staged according to Ludwig:[10]
- Stage 1: Portal - inflammation or bile duct abnormalities.
- Stage 2: Periportal - periportal fibrosis (enlargement of portal tracts) +/- inflammation.
- Stage 3: Septal - septal fibrosis +/-inflammation in septa.
- Stage 4: Cirrhosis - nodules of hepatocytes +/- inflammation.
Notes:
- There can be significant variation in staging on biopsy - due to variability of fibrosis in a PBC liver.[11]
- "Worst area" in biopsy specimen is used to determine stage.
See also
References
- ↑ Beuers U, Gershwin ME, Gish RG, Invernizzi P, Jones DE, Lindor K, Ma X, Mackay IR, Parés A, Tanaka A, Vierling JM, Poupon R (November 2015). "Changing Nomenclature for PBC: From 'Cirrhosis' to 'Cholangitis'". Am J Gastroenterol 110 (11): 1536–8. doi:10.1038/ajg.2015.312. PMC 4679751. PMID 26416194. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4679751/.
- ↑ Tadrous, Paul.J. Diagnostic Criteria Handbook in Histopathology: A Surgical Pathology Vade Mecum (1st ed.). Wiley. pp. 162. ISBN 978-0470519035.
- ↑ Nguyen, DL.; Juran, BD.; Lazaridis, KN. (Oct 2010). "Primary biliary cirrhosis.". Best Pract Res Clin Gastroenterol 24 (5): 647-54. doi:10.1016/j.bpg.2010.07.006. PMID 20955967.
- ↑ Nakanuma, Y.; Harada, K. (Sep 1993). "Florid duct lesion in primary biliary cirrhosis shows highly proliferative activities.". J Hepatol 19 (2): 216-21. PMID 7905494.
- ↑ OA. 11 September 2009.
- ↑ http://dictionary.reference.com/browse/garland
- ↑ Grimm, D.; Thimme, R. (Apr 2011). "[Cholestatic liver diseases].". Ther Umsch 68 (4): 195-9. doi:10.1024/0040-5930/a000150. PMID 21452140.
- ↑ Tadrous, Paul.J. Diagnostic Criteria Handbook in Histopathology: A Surgical Pathology Vade Mecum (1st ed.). Wiley. pp. 163. ISBN 978-0470519035.
- ↑ Vanishing bile duct syndrome and Hodgkin disease: a case series and review of the literature. Pass AK, McLin VA, Rushton JR, Kearney DL, Hastings CA, Margolin JF. J Pediatr Hematol Oncol. 2008 Dec;30(12):976-80. PMID 19131796.
- ↑ PBC. eMedicine.com. URL: http://emedicine.medscape.com/article/171117-diagnosis. Accessed on: 22 September 2009.
- ↑ J Clin Pathol. 1996 July; 49(7): 556-559. Available at: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=500569. Accessed on: September 22, 2009.