Difference between revisions of "Sinus histiocytosis"
Jump to navigation
Jump to search
| (3 intermediate revisions by the same user not shown) | |||
| Line 17: | Line 17: | ||
| Assdx = | | Assdx = | ||
| Syndromes = | | Syndromes = | ||
| Clinicalhx = | | Clinicalhx = variable | ||
| Signs = | | Signs = | ||
| Symptoms = | | Symptoms = | ||
| Line 45: | Line 45: | ||
Features:<ref name=Ref_ILNP179>{{Ref_ILNP|179}}</ref> | Features:<ref name=Ref_ILNP179>{{Ref_ILNP|179}}</ref> | ||
*Sinuses distended with histiocytes - '''key feature'''. | *Sinuses distended with histiocytes - '''key feature'''. | ||
**Histocytes: abundant foamy cytoplasm, +/-[[anthracotic pigment]]. | **Histocytes: abundant foamy cytoplasm, +/-[[anthracotic pigment]] and/or [[yellow bodies]]. | ||
*[[Plasma cell]]s increased. | *[[Plasma cell]]s increased. | ||
| Line 51: | Line 51: | ||
*[[Rosai-Dorfman disease]] - histiocytes have a large round nucleus (~2-3x the size of a lymphocyte) with a prominent nucleolus. | *[[Rosai-Dorfman disease]] - histiocytes have a large round nucleus (~2-3x the size of a lymphocyte) with a prominent nucleolus. | ||
*[[Dermatopathic lymphadenopathy]] - histiocytes have (melanin) pigment. | *[[Dermatopathic lymphadenopathy]] - histiocytes have (melanin) pigment. | ||
*[[Lymph node metastasis]] - usually not difficult if one compares | *[[Lymph node metastasis]] - usually not difficult to exclude, esp. if one compares the germinal center macrophages and the primary tumour. | ||
===Images=== | ===Images=== | ||
Latest revision as of 03:50, 22 October 2014
| Sinus histiocytosis | |
|---|---|
| Diagnosis in short | |
|
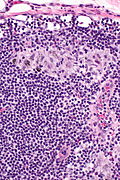
Template:Px Sinus histiocytosis. H&E stain. | |
|
| |
| LM | sinuses distended with histiocytes without atypia |
| LM DDx | Rosai-Dorfman disease, dermatopathic lymphadenopathy, lymph node metastasis |
| IHC | CD68 +ve, S-100 -ve, pankeratin -ve |
| Site | lymph node - see lymph node pathology |
|
| |
| Clinical history | variable |
| Prevalence | common |
| Prognosis | benign |
| Clin. DDx | other causes of lymphadenopathy esp. lymphoma, lymph node metastasis |
Sinus histiocytosis, abbreviated SH, is a common finding in lymph nodes.
It should not be confused with Rosai-Dorfman disease (also known as sinus histiocytosis and massive lymphadenopathy).
General
- Benign.
- Non-specific finding.
- Frequently associated with infections and neoplasia.[1]
- Reported in association with hip replacements.[2]
Gross
- +/-Enlargement of lymph node.[3]
Microscopic
Features:[4]
- Sinuses distended with histiocytes - key feature.
- Histocytes: abundant foamy cytoplasm, +/-anthracotic pigment and/or yellow bodies.
- Plasma cells increased.
DDx:
- Rosai-Dorfman disease - histiocytes have a large round nucleus (~2-3x the size of a lymphocyte) with a prominent nucleolus.
- Dermatopathic lymphadenopathy - histiocytes have (melanin) pigment.
- Lymph node metastasis - usually not difficult to exclude, esp. if one compares the germinal center macrophages and the primary tumour.
Images

SH - intermed. mag.
SH - high mag.
SH - high mag.


IHC
- CD68 +ve.
- S-100 -ve.
- Pankeratin -ve.
- Used to excluded metastatic carcinoma.
Sign out
- The finding is often ignored; may be signed out as morphologically benign lymph nodes.
See also
References
- ↑ Hartmann, S.; Kriener, S.; Hansmann, ML. (Jul 2008). "[Diagnostic spectrum of reactive lymph node changes].". Pathologe 29 (4): 253-63. doi:10.1007/s00292-008-1003-5. PMID 18504582.
- ↑ Albores-Saavedra, J.; Vuitch, F.; Delgado, R.; Wiley, E.; Hagler, H. (Jan 1994). "Sinus histiocytosis of pelvic lymph nodes after hip replacement. A histiocytic proliferation induced by cobalt-chromium and titanium.". Am J Surg Pathol 18 (1): 83-90. PMID 8279630.
- ↑ Saito, T.; Kuwahara, A.; Kaketani, K.; Hirao, E.; Miyahara, M.; Shimoda, K.; Kobayashi, M. (Mar 1991). "Preoperative assessment of cervical lymph node involvement in esophageal cancer.". Jpn J Surg 21 (2): 145-53. PMID 2051659.
- ↑ Ioachim, Harry L; Medeiros, L. Jeffrey (2008). Ioachim's Lymph Node Pathology (4th ed.). Lippincott Williams & Wilkins. pp. 179. ISBN 978-0781775960.