Difference between revisions of "Pediatric gastrointestinal pathology"
(→Meconium ileus: wikify) |
m (→Images) |
||
| (38 intermediate revisions by 3 users not shown) | |||
| Line 6: | Line 6: | ||
==Omphalocele== | ==Omphalocele== | ||
===General=== | ===General=== | ||
Usually genetic (unlike gastroschisis) - associated with:<ref name=pmid20809116>{{Cite journal | last1 = Frolov | first1 = P. | last2 = Alali | first2 = J. | last3 = Klein | first3 = MD. | title = Clinical risk factors for gastroschisis and omphalocele in humans: a review of the literature. | journal = Pediatr Surg Int | volume = 26 | issue = 12 | pages = 1135-48 | month = Dec | year = 2010 | doi = 10.1007/s00383-010-2701-7 | PMID = 20809116 }}</ref> | Usually genetic (unlike [[gastroschisis]]) - associated with:<ref name=pmid20809116>{{Cite journal | last1 = Frolov | first1 = P. | last2 = Alali | first2 = J. | last3 = Klein | first3 = MD. | title = Clinical risk factors for gastroschisis and omphalocele in humans: a review of the literature. | journal = Pediatr Surg Int | volume = 26 | issue = 12 | pages = 1135-48 | month = Dec | year = 2010 | doi = 10.1007/s00383-010-2701-7 | PMID = 20809116 }}</ref> | ||
*[[Trisomy 18]] (Edwards syndrome). | *[[Trisomy 18]] (Edwards syndrome) ~ 6% have omphaloceles in a series of 85 cases.<ref name=pmid3191615>{{Cite journal | last1 = Moore | first1 = CA. | last2 = Harmon | first2 = JP. | last3 = Padilla | first3 = LM. | last4 = Castro | first4 = VB. | last5 = Weaver | first5 = DD. | title = Neural tube defects and omphalocele in trisomy 18. | journal = Clin Genet | volume = 34 | issue = 2 | pages = 98-103 | month = Aug | year = 1988 | doi = | PMID = 3191615 }}</ref> | ||
*[[Beckwith-Wiedemann syndrome]]. | *[[Beckwith-Wiedemann syndrome]]. | ||
Presentation: | Presentation: | ||
*Increased AFP. | *Increased AFP. | ||
===Gross=== | ===Gross=== | ||
*Bowel outside of abdomen - covered by membrane/in a sac. | *Bowel outside of abdomen - covered by membrane/in a sac. | ||
| Line 20: | Line 21: | ||
==Gastroschisis== | ==Gastroschisis== | ||
===General=== | ===General=== | ||
*Defect considered to be more severe than omphalocele. | *Defect considered to be more severe than [[omphalocele]]. | ||
*Usually sporadic. | *Usually sporadic. | ||
| Line 30: | Line 31: | ||
=Luminal pathology= | =Luminal pathology= | ||
==Esophageal atresia== | |||
===General=== | |||
*Multifactoral. | |||
*Often associated with other abnormalities. | |||
Forms:<ref name=pmid17498283>{{Cite journal | last1 = Spitz | first1 = L. | title = Oesophageal atresia. | journal = Orphanet J Rare Dis | volume = 2 | issue = | pages = 24 | month = | year = 2007 | doi = 10.1186/1750-1172-2-24 | PMID = 17498283 }}</ref> | |||
#Esophageal atresia with distal tracheoesophageal fistula - most common. | |||
#Esophageal atresia without a fistula. | |||
Note: | |||
*The "H-type" tracheoeosphageal fistula is often lumped together with ''esophageal atresia''.<ref name=pmid17498283/> | |||
Image: | |||
*[http://commons.wikimedia.org/wiki/File:Atrezja.jpg Esophageal atresia (WC)]. | |||
==Abetalipoproteinemia== | ==Abetalipoproteinemia== | ||
| Line 37: | Line 52: | ||
*Rare genetic disorder.<ref>URL: [http://www.ncbi.nlm.nih.gov/omim/200100 http://www.ncbi.nlm.nih.gov/omim/200100]. Accessed on: 6 April 2011.</ref><ref>{{cite journal |author=Bassen FA, Kornzweig AL |title=Malformation of the erythrocytes in a case of atypical retinitis pigmentosa |journal=Blood |volume=5 |issue=4 |pages=381–87 |year=1950 |month=April |pmid=15411425 |doi= |url=}}</ref> | *Rare genetic disorder.<ref>URL: [http://www.ncbi.nlm.nih.gov/omim/200100 http://www.ncbi.nlm.nih.gov/omim/200100]. Accessed on: 6 April 2011.</ref><ref>{{cite journal |author=Bassen FA, Kornzweig AL |title=Malformation of the erythrocytes in a case of atypical retinitis pigmentosa |journal=Blood |volume=5 |issue=4 |pages=381–87 |year=1950 |month=April |pmid=15411425 |doi= |url=}}</ref> | ||
*GI-related symptoms similar to [[celiac disease]] - malabsorption. | *GI-related symptoms similar to [[celiac disease]] - malabsorption. | ||
Clinical features:<ref name=pmid24139731>{{Cite journal | last1 = Hammer | first1 = MB. | last2 = El Euch-Fayache | first2 = G. | last3 = Nehdi | first3 = H. | last4 = Feki | first4 = M. | last5 = Maamouri-Hicheri | first5 = W. | last6 = Hentati | first6 = F. | last7 = Amouri | first7 = R. | title = Clinical features and molecular genetics of two Tunisian families with abetalipoproteinemia. | journal = J Clin Neurosci | volume = 21 | issue = 2 | pages = 311-5 | month = Feb | year = 2014 | doi = 10.1016/j.jocn.2013.04.016 | PMID = 24139731 }}</ref> | |||
*Failure to thrive. | |||
*Pigmented retinopathy. | |||
Blood work:<ref name=pmid24139731/> | |||
*Cholesterol - low. | |||
*Triglyceride - low. | |||
*Apolipoprotein B - very low. | |||
===Microscopic=== | ===Microscopic=== | ||
| Line 44: | Line 68: | ||
Notes: | Notes: | ||
*Have abnormal erythrocytes with a spiculated cell membranes ''acanthocyte'' - seen on blood films. | *Have abnormal erythrocytes with a spiculated cell membranes ''acanthocyte'' - seen on blood films. | ||
====Images==== | |||
<gallery> | |||
Image:Abetalipoproteinemia_-_intermed_mag.jpg | Abetalipoproteinemia - intermed. mag. (WC) | |||
Image:Abetalipoproteinemia_-_very_high_mag.jpg | Abetalipoproteinemia - very high mag. (WC) | |||
</gallery> | |||
==Microvillous inclusion disease== | ==Microvillous inclusion disease== | ||
| Line 61: | Line 91: | ||
===IHC=== | ===IHC=== | ||
*Carcinoembryonic antigen (CEA) +ve.<ref name=Ref_Sternberg4>{{Ref Sternberg4|}}</ref> | *[[Carcinoembryonic antigen]] (CEA) +ve.<ref name=Ref_Sternberg4>{{Ref Sternberg4|}}</ref> | ||
===EM=== | ===EM=== | ||
| Line 83: | Line 113: | ||
*''Not'' intracellular and extracellular accumulation of mucus. (?) | *''Not'' intracellular and extracellular accumulation of mucus. (?) | ||
== | ==Colonic aganglionosis== | ||
*[[AKA]] Hirschsprung disease. | *[[AKA]] ''Hirschsprung disease''. | ||
===General=== | ===General=== | ||
* | *Genetic disorder:<ref>{{OMIM|142623}}</ref> | ||
* | **5-10% familial; RET gene most commonly mutated. | ||
**Several genes involved. | |||
**Inheritance pattern variable. | |||
*Treatment: surgery (''Swenson's procedure'' or ''Duhamel procedure'').<ref name=pmid6649901>{{Cite journal | last1 = Okasora | first1 = T. | last2 = Okamoto | first2 = E. | last3 = Kuwata | first3 = K. | last4 = Toyosaka | first4 = A. | last5 = Ohashi | first5 = S. | last6 = Ueki | first6 = S. | title = Serum and erythrocyte acetylcholine esterase in Hirschsprung's disease. | journal = Z Kinderchir | volume = 38 | issue = 5 | pages = 298-300 | month = Oct | year = 1983 | doi = 10.1055/s-2008-1059992 | PMID = 6649901 }}</ref> | |||
Pathology: | Pathology: | ||
*Parasympathetic ganglion cells in | *Failure of neural crest cell migration | ||
**Parasympathetic ganglion cells in submucosal plexus (Meissner plexus) and myenteric plexus (Auerbach plexus) - absent.<ref name=pmid17139897>{{Cite journal | last1 = Vorobyov | first1 = GI. | last2 = Achkasov | first2 = SI. | last3 = Biryukov | first3 = OM. | title = Hirschsprung's disease in adults. | journal = Acta Chir Iugosl | volume = 53 | issue = 2 | pages = 113-6 | month = | year = 2006 | doi = | PMID = 17139897 }}</ref> | |||
Notes: | Notes: | ||
*Most common reason for litigation in paediatric pathology.<ref> | *Most common reason for litigation in paediatric pathology.<ref>Taylor, G. 19 January 2011.</ref> | ||
===Gross=== | |||
Features: | |||
*Dilated bowel; stuffed sausage-look. | |||
Classification: | |||
*Short-segment (75-80%): Rectum, distal sigmoid | |||
*Long-segment HD (10-20%): Beyond splenic flexure | |||
*Total colonic aganglionosis (5-15%): Entire colon.<ref name=pmid25395999>{{Cite web | last = | first = | title = Diagnosis of Hirschsprung's disease with particular emphasis on histopathology. A systematic review of current literature | url = https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4223113/ | publisher = | date = | accessdate = 19 August 2017 }}</ref> | |||
**[https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4223113/figure/F0001/ Classification of Hirschsprung's disease according to the aganglionic segment length (https://www.ncbi.nlm.nih.gov)] | |||
Image: | |||
*[http://www.pathology.pitt.edu/lectures/gi/colon-a/03.htm Hirschsprung disease (pathology.pitt.edu)]. | |||
===Microscopic=== | ===Microscopic=== | ||
Features: | Features: | ||
*Ganglion cells missing in submucosal plexus and myenteric plexus. | *Ganglion cells missing in submucosal plexus and myenteric plexus. | ||
**Increasing ganglia proximally into transition zone | |||
*Hypertrophy of neural plexuses. | |||
**Many nerve trunks > 40 μm | |||
*Abnormal submucosal blood vessels may be seen | |||
*+/-Submucosal fibrosis. | *+/-Submucosal fibrosis. | ||
Image: | |||
*[http://pathology.mc.duke.edu/research/Histo_course/myent_plexus.jpg Normal myenteric plexus (duke.edu)].<ref>URL: [http://pathology.mc.duke.edu/research/PTH225.html http://pathology.mc.duke.edu/research/PTH225.html]. Accessed on: 11 January 2011.</ref> | |||
===Stains=== | ===Stains=== | ||
*Acetylcholinesterase | *Acetylcholinesterase - marks the abundant, disorganized, nerve fibers. | ||
* | |||
Image: | |||
*[http://commons.wikimedia.org/wiki/File:Hirschsprung_acetylcholine.jpg Hirschsprung - acetylcholinesterase (WC)]. | |||
===IHC=== | |||
Features:<ref name=pmid1640323>{{Cite journal | last1 = Luider | first1 = TM. | last2 = van Dommelen | first2 = MW. | last3 = Tibboel | first3 = D. | last4 = Meijers | first4 = JH. | last5 = Ten Kate | first5 = FJ. | last6 = Trojanowski | first6 = JQ. | last7 = Molenaar | first7 = JC. | title = Differences in phosphorylation state of neurofilament proteins in ganglionic and aganglionic bowel segments of children with Hirschsprung's disease. | journal = J Pediatr Surg | volume = 27 | issue = 7 | pages = 815-9 | month = Jul | year = 1992 | doi = | PMID = 1640323 }}</ref> | |||
* | *NF-M (neurofilament middle) - highlight hypertrophic nerve fascicules | ||
*NF-H (neurofilament high) - highlight hypertrophic nerve fascicules. | |||
*Tau ~ highlights ganglion cells (which are absent in segments affected by Hirschsprung).<ref name=pmid8229560>{{Cite journal | last1 = Deguchi | first1 = E. | last2 = Iwai | first2 = N. | last3 = Goto | first3 = Y. | last4 = Yanagihara | first4 = J. | last5 = Fushiki | first5 = S. | title = An immunohistochemical study of neurofilament and microtubule-associated Tau protein in the enteric innervation in Hirschsprung's disease. | journal = J Pediatr Surg | volume = 28 | issue = 7 | pages = 886-90 | month = Jul | year = 1993 | doi = | PMID = 8229560 }}</ref> | |||
**Nerve fibres +ve control. | |||
Others<ref>{{Cite book | last1 = Lin | first1 = Fan | last2 = Prichard | first2 = Jeffrey | title = Handbook of practical immunohistochemistry : frequently asked question | date = | publisher = | location = | isbn = 9781493915774 | pages = }}</ref> | |||
: | |||
*Calretinin ~ -ve, Usually negative in hypertrophied nerve fibers in Hirschsprung’s disease, superior to acetylcholinesterase. | |||
*NSE ~ -ve, Highlights ganglion cells to exclude Hirschsprung’s disease; specific but not very sensitive. | |||
==Meconium ileus== | ==Meconium ileus== | ||
| Line 112: | Line 177: | ||
*Classically due to ''[[cystic fibrosis]]''. | *Classically due to ''[[cystic fibrosis]]''. | ||
*May lead to ''[[meconium peritonitis]]''. | *May lead to ''[[meconium peritonitis]]''. | ||
*Can be mimicked by [[CMV]] infection.<ref>{{cite journal |author=Déchelotte PJ, Mulliez NM, Bouvier RJ, Vanlieféringhen PC, Lémery DJ |title=Pseudo-meconium ileus due to cytomegalovirus infection: a report of three cases |journal=Pediatr Pathol |volume=12 |issue=1 |pages=73–82 |year=1992 |pmid=1313975 |doi= |url=}}</ref> | |||
===Gross=== | ===Gross=== | ||
| Line 119: | Line 185: | ||
*Green. | *Green. | ||
Image | ====Image==== | ||
*[http://library.med.utah.edu/WebPath/jpeg3/PERI175.jpg Meconium ileus (med.utah.edu)].<ref>URL: [http://library.med.utah.edu/WebPath/EXAM/IMGQUIZ/pdfrm.html http://library.med.utah.edu/WebPath/EXAM/IMGQUIZ/pdfrm.html]. Accessed on: 3 December 2011.</ref> | *[http://library.med.utah.edu/WebPath/jpeg3/PERI175.jpg Meconium ileus (med.utah.edu)].<ref>URL: [http://library.med.utah.edu/WebPath/EXAM/IMGQUIZ/pdfrm.html http://library.med.utah.edu/WebPath/EXAM/IMGQUIZ/pdfrm.html]. Accessed on: 3 December 2011.</ref> | ||
| Line 154: | Line 220: | ||
Features: | Features: | ||
*Large spaces. | *Large spaces. | ||
DDx: | |||
*[[Pneumatosis intestinalis]]. | |||
Images: | Images: | ||
*[http://en.wikipedia.org/wiki/File:Neonatal_necrotizing_enterocolitis,_gross_pathology_20G0021_lores.jpg NEC - gross (WP)]. | *[http://en.wikipedia.org/wiki/File:Neonatal_necrotizing_enterocolitis,_gross_pathology_20G0021_lores.jpg NEC - gross (WP)]. | ||
*[ | *[https://library.med.utah.edu/WebPath/PEDHTML/PED045.html NEC - micro]. | ||
==Autoimmune enteropathy== | ==Autoimmune enteropathy== | ||
| Line 203: | Line 272: | ||
*Lobular cholestasis. | *Lobular cholestasis. | ||
Images | ====Images==== | ||
==Biliary atresia== | ==Biliary atresia== | ||
Latest revision as of 18:35, 6 May 2018
This article deals with pediatric gastrointestinal pathology. An introduction to pediatric pathology is in the pediatric pathology article.
An overview of (adult) gastrointestinal pathology is in the gastrointestinal pathology article.
Birth defects
Omphalocele
General
Usually genetic (unlike gastroschisis) - associated with:[1]
- Trisomy 18 (Edwards syndrome) ~ 6% have omphaloceles in a series of 85 cases.[2]
- Beckwith-Wiedemann syndrome.
Presentation:
- Increased AFP.
Gross
- Bowel outside of abdomen - covered by membrane/in a sac.
Image:
Gastroschisis
General
- Defect considered to be more severe than omphalocele.
- Usually sporadic.
Gross
- Bowel outside of abdomen - individual loops of bowel are seen.
Image:
Luminal pathology
Esophageal atresia
General
- Multifactoral.
- Often associated with other abnormalities.
Forms:[3]
- Esophageal atresia with distal tracheoesophageal fistula - most common.
- Esophageal atresia without a fistula.
Note:
- The "H-type" tracheoeosphageal fistula is often lumped together with esophageal atresia.[3]
Image:
Abetalipoproteinemia
- AKA Bassen-Kornzweig syndrome.
General
- Rare genetic disorder.[4][5]
- GI-related symptoms similar to celiac disease - malabsorption.
Clinical features:[6]
- Failure to thrive.
- Pigmented retinopathy.
Blood work:[6]
- Cholesterol - low.
- Triglyceride - low.
- Apolipoprotein B - very low.
Microscopic
Features:
- Enterocytes have clear cytoplasm (due to lipid accumulation).
Notes:
- Have abnormal erythrocytes with a spiculated cell membranes acanthocyte - seen on blood films.
Images

Abetalipoproteinemia - intermed. mag. (WC)
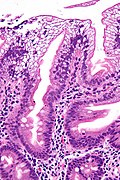
Abetalipoproteinemia - very high mag. (WC)


{kind=link}
Microvillous inclusion disease
- AKA Davidson disease.
General
- Autosomal recessive inherited condition - due to mutation in MYO5B.[7]
Microscopic
Features:
- Flat mucosa; no villi.
Notes:
- Appearance similar to celiac sprue; however, usually lacks the intraepithelial lymphocytic infiltration characteristic of celiac sprue.
Images:
IHC
- Carcinoembryonic antigen (CEA) +ve.[8]
EM
- Diagnosis is dependent on electron microscopy.[9]
Images:
Cystic fibrosis
General
- Genetic.
- May lead to meconium ileus.
Microscopic
Features - large bowel:[10]
- Crypt enlargement.
Notes:
- Not intracellular and extracellular accumulation of mucus. (?)
Colonic aganglionosis
- AKA Hirschsprung disease.
General
- Genetic disorder:[11]
- 5-10% familial; RET gene most commonly mutated.
- Several genes involved.
- Inheritance pattern variable.
- Treatment: surgery (Swenson's procedure or Duhamel procedure).[12]
Pathology:
- Failure of neural crest cell migration
- Parasympathetic ganglion cells in submucosal plexus (Meissner plexus) and myenteric plexus (Auerbach plexus) - absent.[13]
Notes:
- Most common reason for litigation in paediatric pathology.[14]
Gross
Features:
- Dilated bowel; stuffed sausage-look.
Classification:
- Short-segment (75-80%): Rectum, distal sigmoid
- Long-segment HD (10-20%): Beyond splenic flexure
- Total colonic aganglionosis (5-15%): Entire colon.[15]
Image:
Microscopic
Features:
- Ganglion cells missing in submucosal plexus and myenteric plexus.
- Increasing ganglia proximally into transition zone
- Hypertrophy of neural plexuses.
- Many nerve trunks > 40 μm
- Abnormal submucosal blood vessels may be seen
- +/-Submucosal fibrosis.
Image:
{kind=link}
Stains
- Acetylcholinesterase - marks the abundant, disorganized, nerve fibers.
Image:
{kind=link}
IHC
Features:[17]
- NF-M (neurofilament middle) - highlight hypertrophic nerve fascicules
- NF-H (neurofilament high) - highlight hypertrophic nerve fascicules.
- Tau ~ highlights ganglion cells (which are absent in segments affected by Hirschsprung).[18]
- Nerve fibres +ve control.
Others[19]
- Calretinin ~ -ve, Usually negative in hypertrophied nerve fibers in Hirschsprung’s disease, superior to acetylcholinesterase.
- NSE ~ -ve, Highlights ganglion cells to exclude Hirschsprung’s disease; specific but not very sensitive.
Meconium ileus
General
- Classically due to cystic fibrosis.
- May lead to meconium peritonitis.
- Can be mimicked by CMV infection.[20]
Gross
Features:
- Thick.
- High viscosity.
- Green.
Image
{kind=link}
Microscopic
Features:
- Meconium-laden macrophages. (???)
Meconium peritonitis
General
- May be due to a number of causes:
- Aganglionosis (Hirschsprung disease).
- Meconium ileus.
Microscopic
Features:
- Brown granular material - key feature.
- +/-Multinucleated giant cells.
- Inflammatory infiltrate (PMNs, lymphocytes, plasma cells).
Image:
{kind=link}
Necrotizing enterocolitis
- Abbreviated NEC.
General
- Disease primarily of premature babies.
- Diagnosed by imaging.
Note:
- Enterocolitis = inflammation of small bowel and colon.[22]
- Necrotizing enteritis = small bowel only.
Microscopic
Features:
- Large spaces.
DDx:
Images:
{kind=link}
Autoimmune enteropathy
Pancreas
Pancreatic islet cell hyperplasia
General
- Associated with maternal diabetes.
Microscopic
Features:
- Marked size variation of pancreatic islets.
- Normal islets ~ 150 micrometers (diameter). Hyperplastic islets - up to ~500 micrometers (diameter).
Image:
Liver
Giant cell hepatitis
- AKA neonatal giant cell hepatitis, abbreviated NGCH.
General
- Rare.
Etiology:
- Unknown - possibly viral, autoimmune and/or drugs.[23]
- One large series suggests that, in the neonatal population, with follow-up the causes are:
- ~49% idiopathic.
- ~16% pan-hypopituitarism.
- ~8% biliary atresia.
- ~6% Alagille syndrome
- ~6% bile salt defects.
Notes:
- May be seen in adults.[24]
- Reported association with subdural hematoma.[25]
Microscopic
Features:[26]
- Giant hepatocytes with multiple nuclei - key feature.
- Typically ~35% of hepatocytes affected.
- Minimal or absent inflammation portal and lobular inflammation.
- Lobular cholestasis.
Images
Biliary atresia
General
- 1/3 of neonatal cholestasis.[27]
- Etiology - various.
Microscopic
Features:[27]
- Bile duct proliferation.
- Portal tract edema.
- Portal tract fibrosis.
Image:
See also
References
- ↑ Frolov, P.; Alali, J.; Klein, MD. (Dec 2010). "Clinical risk factors for gastroschisis and omphalocele in humans: a review of the literature.". Pediatr Surg Int 26 (12): 1135-48. doi:10.1007/s00383-010-2701-7. PMID 20809116.
- ↑ Moore, CA.; Harmon, JP.; Padilla, LM.; Castro, VB.; Weaver, DD. (Aug 1988). "Neural tube defects and omphalocele in trisomy 18.". Clin Genet 34 (2): 98-103. PMID 3191615.
- ↑ 3.0 3.1 Spitz, L. (2007). "Oesophageal atresia.". Orphanet J Rare Dis 2: 24. doi:10.1186/1750-1172-2-24. PMID 17498283.
- ↑ URL: http://www.ncbi.nlm.nih.gov/omim/200100. Accessed on: 6 April 2011.
- ↑ Bassen FA, Kornzweig AL (April 1950). "Malformation of the erythrocytes in a case of atypical retinitis pigmentosa". Blood 5 (4): 381–87. PMID 15411425.
- ↑ 6.0 6.1 Hammer, MB.; El Euch-Fayache, G.; Nehdi, H.; Feki, M.; Maamouri-Hicheri, W.; Hentati, F.; Amouri, R. (Feb 2014). "Clinical features and molecular genetics of two Tunisian families with abetalipoproteinemia.". J Clin Neurosci 21 (2): 311-5. doi:10.1016/j.jocn.2013.04.016. PMID 24139731.
- ↑ Müller T, Hess MW, Schiefermeier N, et al. (October 2008). "MYO5B mutations cause microvillus inclusion disease and disrupt epithelial cell polarity". Nat. Genet. 40 (10): 1163–5. doi:10.1038/ng.225. PMID 18724368.
- ↑ Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Oberman, Harold A; Reuter, Victor E (2004). Sternberg's Diagnostic Surgical Pathology (4th ed.). Lippincott Williams & Wilkins. ISBN 978-0781740517.
- ↑ Kennea N, Norbury R, Anderson G, Tekay A (2001). "Congenital microvillous inclusion disease presenting as antenatal bowel obstruction". Ultrasound Obstet Gynecol 17 (2): 172–4. doi:10.1046/j.1469-0705.2001.00211.x. PMID 11251929.
- ↑ Neutra MR, Trier JS (October 1978). "Rectal mucosa in cystic fibrosis. Morphological features before and after short term organ culture". Gastroenterology 75 (4): 701–10. PMID 710839.
- ↑ Online 'Mendelian Inheritance in Man' (OMIM) 142623
- ↑ Okasora, T.; Okamoto, E.; Kuwata, K.; Toyosaka, A.; Ohashi, S.; Ueki, S. (Oct 1983). "Serum and erythrocyte acetylcholine esterase in Hirschsprung's disease.". Z Kinderchir 38 (5): 298-300. doi:10.1055/s-2008-1059992. PMID 6649901.
- ↑ Vorobyov, GI.; Achkasov, SI.; Biryukov, OM. (2006). "Hirschsprung's disease in adults.". Acta Chir Iugosl 53 (2): 113-6. PMID 17139897.
- ↑ Taylor, G. 19 January 2011.
- ↑ "Diagnosis of Hirschsprung's disease with particular emphasis on histopathology. A systematic review of current literature". https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4223113/. Retrieved 19 August 2017.
- ↑ URL: http://pathology.mc.duke.edu/research/PTH225.html. Accessed on: 11 January 2011.
- ↑ Luider, TM.; van Dommelen, MW.; Tibboel, D.; Meijers, JH.; Ten Kate, FJ.; Trojanowski, JQ.; Molenaar, JC. (Jul 1992). "Differences in phosphorylation state of neurofilament proteins in ganglionic and aganglionic bowel segments of children with Hirschsprung's disease.". J Pediatr Surg 27 (7): 815-9. PMID 1640323.
- ↑ Deguchi, E.; Iwai, N.; Goto, Y.; Yanagihara, J.; Fushiki, S. (Jul 1993). "An immunohistochemical study of neurofilament and microtubule-associated Tau protein in the enteric innervation in Hirschsprung's disease.". J Pediatr Surg 28 (7): 886-90. PMID 8229560.
- ↑ Lin, Fan; Prichard, Jeffrey. Handbook of practical immunohistochemistry : frequently asked question. ISBN 9781493915774.
- ↑ Déchelotte PJ, Mulliez NM, Bouvier RJ, Vanlieféringhen PC, Lémery DJ (1992). "Pseudo-meconium ileus due to cytomegalovirus infection: a report of three cases". Pediatr Pathol 12 (1): 73–82. PMID 1313975.
- ↑ URL: http://library.med.utah.edu/WebPath/EXAM/IMGQUIZ/pdfrm.html. Accessed on: 3 December 2011.
- ↑ URL: http://medical-dictionary.thefreedictionary.com/enterocolitis. Accessed on: 10 October 2011.
- ↑ Hartl, J.; Buettner, R.; Rockmann, F.; Farkas, S.; Holstege, A.; Vogel, C.; Schnitzbauer, A.; Schlitt, HJ. et al. (Nov 2010). "Giant cell hepatitis: an unusual cause of fulminant liver failure.". Z Gastroenterol 48 (11): 1293-6. doi:10.1055/s-0029-1245476. PMID 21043007.
- ↑ Hayashi, H.; Narita, R.; Hiura, M.; Abe, S.; Tabaru, A.; Tanimoto, A.; Sasaguri, Y.; Harada, M. (2011). "A case of adult autoimmune hepatitis with histological features of giant cell hepatitis.". Intern Med 50 (4): 315-9. PMID 21325763.
- ↑ Guddat, SS.; Ehrlich, E.; Martin, H.; Tsokos, M. (Sep 2011). "Fatal spontaneous subdural bleeding due to neonatal giant cell hepatitis: a rare differential diagnosis of shaken baby syndrome.". Forensic Sci Med Pathol 7 (3): 294-7. doi:10.1007/s12024-011-9227-8. PMID 21331818.
- ↑ Torbenson, M.; Hart, J.; Westerhoff, M.; Azzam, RK.; Elgendi, A.; Mziray-Andrew, HC.; Kim, GE.; Scheimann, A. (Oct 2010). "Neonatal giant cell hepatitis: histological and etiological findings.". Am J Surg Pathol 34 (10): 1498-503. doi:10.1097/PAS.0b013e3181f069ab. PMID 20871223.
- ↑ 27.0 27.1 Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 464. ISBN 978-1416054542.
- ↑ Hertel, PM.; Estes, MK. (Jan 2012). "Rotavirus and biliary atresia: can causation be proven?". Curr Opin Gastroenterol 28 (1): 10-7. doi:10.1097/MOG.0b013e32834c7ae4. PMID 22123643.
- ↑ Santos, JL.; Choquette, M.; Bezerra, JA. (Feb 2010). "Cholestatic liver disease in children.". Curr Gastroenterol Rep 12 (1): 30-9. doi:10.1007/s11894-009-0081-8. PMID 20425482.