Difference between revisions of "Endocervical adenocarcinoma in situ"
(redirect to the histology article) |
(→Microscopic: Put in ioffe scoring system) |
||
| (8 intermediate revisions by one other user not shown) | |||
| Line 1: | Line 1: | ||
# | {{ Infobox diagnosis | ||
| Name = {{PAGENAME}} | |||
| Image = Endocervical adenocarcinoma in situ -- very high mag.jpg | |||
| Width = | |||
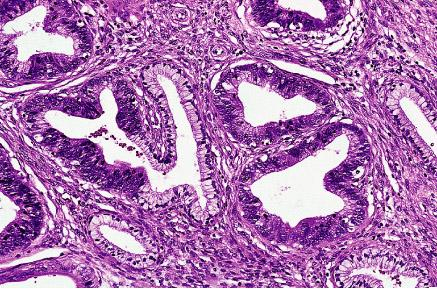
| Caption = Endocervical adenocarcinoma in situ. [[H&E stain]]. | |||
| Synonyms = | |||
| Micro = Nuclear changes (nuclear crowding/pseudostratification, nuclear enlargement (often cigar-shaped nuclei), coarse chromatin, small nucleolus or nucleoli), +/-mitoses, +/-reduced cytoplasmic mucin, preservation of glandular architecture | |||
| Subtypes = | |||
| LMDDx = [[Tubal metaplasia of the uterine cervix|tubal metaplasia]], [[Arias-Stella reaction]], [[endometriosis]], lower uterine segment epithelium (esp. [[proliferative phase endometrium]]), [[endocervical adenocarcinoma]], [[metastasis|metastatic]] adenocarcinoma | |||
| Stains = | |||
| IHC = p16 +ve | |||
| EM = | |||
| Molecular = | |||
| IF = | |||
| Gross = | |||
| Grossing = | |||
| Site = [[uterine cervix]] - endocervical canal | |||
| Assdx = squamous lesions ([[LSIL]], [[HSIL]]) | |||
| Syndromes = | |||
| Clinicalhx = +/-[[HPV]] | |||
| Signs = | |||
| Symptoms = asymptomatic | |||
| Prevalence = uncommon | |||
| Bloodwork = | |||
| Rads = | |||
| Endoscopy = | |||
| Prognosis = | |||
| Other = | |||
| ClinDDx = [[endocervical adenocarcinoma]] (invasive), [[endometrial carcinoma]], squamous cervical lesions | |||
| Tx = typically [[LEEP]] | |||
}} | |||
:''For the cytology see [[Gynecologic cytopathology#Endocervical adenocarcinoma in situ|Endocervical adenocarcinoma in situ (cytology)]]'' | |||
'''Endocervical adenocarcinoma in situ''', also '''adenocarcinoma in situ of the uterine endocervix''', is pre-invasive change of the [[uterine cervix|uterine endocervix]]. It is closely tied to [[HPV]] infection. | |||
If the context is clear, it may be referred to as '''[[adenocarcinoma in situ]]''', abbreviated '''AIS'''. | |||
==General== | |||
*Usually due to [[HPV]]. | |||
*May be found together with squamous neoplasias of the cervix. | |||
*AIS of the cervix is much less common than squamous dysplasia of the cervix/SCC of the cervix. | |||
*Generally, definitely diagnosed with an ''endocervical curettage'' (ECC). | |||
==Gross== | |||
*Not apparent at colposcopy. | |||
==Microscopic== | |||
Features:<ref name=pmid10757337>{{Cite journal | last1 = Zaino | first1 = RJ. | title = Glandular lesions of the uterine cervix. | journal = Mod Pathol | volume = 13 | issue = 3 | pages = 261-74 | month = Mar | year = 2000 | doi = 10.1038/modpathol.3880047 | PMID = 10757337 | url = http://www.nature.com/modpathol/journal/v13/n3/full/3880047a.html }}</ref> | |||
#Nuclear changes - '''key feature''': | |||
#*Variable nuclear stratification. | |||
#**Nuclear crowding/pseudostratification. | |||
#*Nuclear enlargement. | |||
#**Often cigar-shaped nuclei. | |||
#*Coarse chromatin. | |||
#*Small nucleolus or [[nucleoli]]. | |||
#+/-Mitoses. | |||
#+/-Reduced cytoplasmic mucin. | |||
#Preservation of glandular architecture. | |||
#*Normal gland spacing - lack of complexity ("lobular pattern"). | |||
#*Normal gland depth (subjective). | |||
Ioffe, et al, :<ref name=pmid12657929>{{cite journal |author=Ioffe OB, Sagae S, Moritani S, Dahmoush L, Chen TT, Silverberg SG. |title=Proposal of a new scoring scheme for the diagnosis of noninvasive endocervical glandular lesions |journal=Am J Surg Pathol | volume=27 | issue=4| pages=452–460 | year=2003 | pmid=12657929 |pmc= |doi= |url= }}</ref> devised a reproducible schema by which one might discern reactive glandular atypia, glandular dysplasia, and adenocarcinoma in situ, summarized in the table below from the article: | |||
Sum the scores for stratification, nuclear atypia, and mitoses/apoptotic bodies<br> | |||
<br> | |||
Stratification<br> | |||
None (0 points)<br> | |||
Mild (1 point)<br> | |||
Moderate (2 points)<br> | |||
Up to the luminal surface (3 points)<br> | |||
<br> | |||
Nuclear atypia<br> | |||
As normal (0 points)<br> | |||
Small (size of normal) or slightly enlarged uniform nuclei, minimal hyperchromasia, little dispolarity, no nucleoli (1 point)<br> | |||
Nuclear enlargement (≤3× normal), moderate anisocytosis/hyperchromasia/dispolarity, occasional small nucleoli (2 points)<br> | |||
Large nuclei (>3× normal), marked anisocytosis, marked hyperchromasia, severe dispolarity, frequent prominent nucleoli (3 points)<br> | |||
<br> | |||
Mitoses and apoptoses in two most active glands, number per gland (average between two glands)<br> | |||
None (0 points)<br> | |||
Less than 0.5 per gland (1 point)<br> | |||
0.6–3.0 per gland (2 points)<br> | |||
>3.0 per gland (3 points)<br> | |||
<br> | |||
Total score 0–3 = benign 4–5 = endocervical glandular dysplasia (EGD) 6–9 = adenocarcinoma in situ | |||
DDx: | |||
*[[Tubal metaplasia of the uterine cervix|Tubal metaplasia]]. | |||
*[[Arias-Stella reaction]]. | |||
*[[Endometriosis]]. | |||
*Lower uterine segment epithelium<ref name=Ref_GP167>{{Ref GP|167}}</ref> - esp. [[proliferative phase endometrium]] - mitoses rare, NC ratio normal, stroma different. | |||
*[[Endocervical adenocarcinoma]] - often has paradoxical maturation... paler cytoplasm & nuclei than adjacent AIS. | |||
*[[metastasis|Metastatic]] adenocarcinoma. | |||
*[[Proliferative phase endometrium]] - endometrial type stroma, cytoplasm not pale staining, no nuclear atypia (smooth nuclear contour, stratified). | |||
===Images=== | |||
====Case - ECC==== | |||
<gallery> | |||
Image: Endocervical adenocarcinoma in situ -- intermed mag.jpg | AIS - intermed. mag. | |||
Image: Endocervical adenocarcinoma in situ -- high mag.jpg | AIS - high mag. | |||
Image: Endocervical adenocarcinoma in situ -- very high mag.jpg | AIS - very high mag. | |||
Image: Endocervical adenocarcinoma in situ 2 -- intermed mag.jpg | AIS - intermed. mag. | |||
Image: Endocervical adenocarcinoma in situ 2 -- high mag.jpg | AIS - high mag. | |||
Image: Endocervical adenocarcinoma in situ 2a -- very high mag.jpg | AIS - very high mag. | |||
Image: Endocervical adenocarcinoma in situ 2b -- very high mag.jpg | AIS - very high mag. | |||
</gallery> | |||
====Case - biopsy==== | |||
<gallery> | |||
Image: Endocervical adenocarcinoma in situ --- intermed mag.jpg | AIS - intermed. mag. | |||
Image: Endocervical adenocarcinoma in situ --- high mag.jpg | AIS - high mag. | |||
Image: Endocervical adenocarcinoma in situ --- very high mag.jpg | AIS - very high mag. | |||
Image: Endocervical adenocarcinoma in situ - alt --- intermed mag.jpg | AIS - intermed. mag. | |||
Image: Endocervical adenocarcinoma in situ - alt --- high mag.jpg | AIS - high mag. | |||
Image: Endocervical adenocarcinoma in situ - alt --- very high mag.jpg | AIS - very high mag. | |||
Image: Endocervical adenocarcinoma in situ - p16 --- intermed mag.jpg | AIS - p16 - intermed. mag. | |||
Image: Endocervical adenocarcinoma in situ - p16 --- high mag.jpg | AIS - p16 - high mag. | |||
Image: Endocervical adenocarcinoma in situ - p16 --- very high mag.jpg | AIS - p16 - very high mag. | |||
Image: Endocervical adenocarcinoma in situ - ki67 --- intermed mag.jpg | AIS - Ki-67 - intermed. mag. | |||
Image: Endocervical adenocarcinoma in situ - ki67 --- high mag.jpg | AIS - Ki-67 - high mag. | |||
Image: Endocervical adenocarcinoma in situ - ki67 --- very high mag.jpg | AIS - Ki-67 - very high mag. | |||
</gallery> | |||
====www==== | |||
*[https://www.flickr.com/photos/euthman/1799754415 Endocervical AIS adjacent to normal (flickr.com/euthman)]. | |||
*[http://nih.techriver.net/view.php?patientId=99 Endocervical adenocarcinoma in situ (techriver.net)]. | |||
*[http://womenshealthsection.com/content/gynpc/gynpc006d.jpg Endocervical adenocarcinoma in situ (womenshealthsection.com)].<ref>URL: [http://www.womenshealthsection.com/content/print.php3?title=gynpc006&cat=60&lng=english http://www.womenshealthsection.com/content/print.php3?title=gynpc006&cat=60&lng=english]. Accessed on: 20 March 2013.</ref> | |||
*[http://nih.techriver.net/view.php?patientId=67 Endocervical adenocarcinoma in situ - cytology (techriver.net)]. | |||
==IHC== | |||
*p16 +ve. | |||
*CEA +ve. | |||
*Vimentin -ve. | |||
==Sign out== | |||
<pre> | |||
UTERINE CERVIX, BIOPSY: | |||
- HIGH-GRADE SQUAMOUS INTRAEPITHELIAL LESION (HSIL). | |||
- ENDOCERVICAL ADENOCARCINOMA IN SITU (AIS). | |||
- ACUTE AND CHRONIC INFLAMMATION. | |||
COMMENT: | |||
A p16 immunostain marks the full thickness of the squamous epithelium and is | |||
strong. A Ki-67 immunostain marks increased numbers of superficial squamous cells. | |||
The atypical endocervical epithelium (interpreted as AIS) is strongly p16 positive | |||
and has an increased proliferative activity with Ki-67 staining. | |||
</pre> | |||
===Micro=== | |||
The atypical endocervical epithelium (interpreted as AIS) shows marked hyperchromasia, nuclear crowding and moderate nuclear atypia with a relatively abundant cytoplasm ( nucleus to cell size = 1:2 ). | |||
==See also== | |||
*[[Endocervical adenocarcinoma]]. | |||
*[[Uterine cervix]]. | |||
==References== | |||
{{Reflist|2}} | |||
[[Category:Diagnosis]] | [[Category:Diagnosis]] | ||
[[Category:Uterine cervix]] | |||
Latest revision as of 18:38, 14 February 2017
| Endocervical adenocarcinoma in situ | |
|---|---|
| Diagnosis in short | |
|
Template:Px Endocervical adenocarcinoma in situ. H&E stain. | |
|
| |
| LM | Nuclear changes (nuclear crowding/pseudostratification, nuclear enlargement (often cigar-shaped nuclei), coarse chromatin, small nucleolus or nucleoli), +/-mitoses, +/-reduced cytoplasmic mucin, preservation of glandular architecture |
| LM DDx | tubal metaplasia, Arias-Stella reaction, endometriosis, lower uterine segment epithelium (esp. proliferative phase endometrium), endocervical adenocarcinoma, metastatic adenocarcinoma |
| IHC | p16 +ve |
| Site | uterine cervix - endocervical canal |
|
| |
| Associated Dx | squamous lesions (LSIL, HSIL) |
| Clinical history | +/-HPV |
| Symptoms | asymptomatic |
| Prevalence | uncommon |
| Clin. DDx | endocervical adenocarcinoma (invasive), endometrial carcinoma, squamous cervical lesions |
| Treatment | typically LEEP |
{kind=link}
- For the cytology see Endocervical adenocarcinoma in situ (cytology)
Endocervical adenocarcinoma in situ, also adenocarcinoma in situ of the uterine endocervix, is pre-invasive change of the uterine endocervix. It is closely tied to HPV infection.
If the context is clear, it may be referred to as adenocarcinoma in situ, abbreviated AIS.
General
- Usually due to HPV.
- May be found together with squamous neoplasias of the cervix.
- AIS of the cervix is much less common than squamous dysplasia of the cervix/SCC of the cervix.
- Generally, definitely diagnosed with an endocervical curettage (ECC).
Gross
- Not apparent at colposcopy.
Microscopic
Features:[1]
- Nuclear changes - key feature:
- Variable nuclear stratification.
- Nuclear crowding/pseudostratification.
- Nuclear enlargement.
- Often cigar-shaped nuclei.
- Coarse chromatin.
- Small nucleolus or nucleoli.
- Variable nuclear stratification.
- +/-Mitoses.
- +/-Reduced cytoplasmic mucin.
- Preservation of glandular architecture.
- Normal gland spacing - lack of complexity ("lobular pattern").
- Normal gland depth (subjective).
Ioffe, et al, :[2] devised a reproducible schema by which one might discern reactive glandular atypia, glandular dysplasia, and adenocarcinoma in situ, summarized in the table below from the article:
Sum the scores for stratification, nuclear atypia, and mitoses/apoptotic bodies
Stratification
None (0 points)
Mild (1 point)
Moderate (2 points)
Up to the luminal surface (3 points)
Nuclear atypia
As normal (0 points)
Small (size of normal) or slightly enlarged uniform nuclei, minimal hyperchromasia, little dispolarity, no nucleoli (1 point)
Nuclear enlargement (≤3× normal), moderate anisocytosis/hyperchromasia/dispolarity, occasional small nucleoli (2 points)
Large nuclei (>3× normal), marked anisocytosis, marked hyperchromasia, severe dispolarity, frequent prominent nucleoli (3 points)
Mitoses and apoptoses in two most active glands, number per gland (average between two glands)
None (0 points)
Less than 0.5 per gland (1 point)
0.6–3.0 per gland (2 points)
>3.0 per gland (3 points)
Total score 0–3 = benign 4–5 = endocervical glandular dysplasia (EGD) 6–9 = adenocarcinoma in situ
DDx:
- Tubal metaplasia.
- Arias-Stella reaction.
- Endometriosis.
- Lower uterine segment epithelium[3] - esp. proliferative phase endometrium - mitoses rare, NC ratio normal, stroma different.
- Endocervical adenocarcinoma - often has paradoxical maturation... paler cytoplasm & nuclei than adjacent AIS.
- Metastatic adenocarcinoma.
- Proliferative phase endometrium - endometrial type stroma, cytoplasm not pale staining, no nuclear atypia (smooth nuclear contour, stratified).
Images
Case - ECC
AIS - intermed. mag.
AIS - high mag.
- Endocervical adenocarcinoma in situ -- very high mag.jpg
AIS - very high mag.
- Endocervical adenocarcinoma in situ 2 -- intermed mag.jpg
AIS - intermed. mag.
- Endocervical adenocarcinoma in situ 2 -- high mag.jpg
AIS - high mag.
- Endocervical adenocarcinoma in situ 2a -- very high mag.jpg
AIS - very high mag.
- Endocervical adenocarcinoma in situ 2b -- very high mag.jpg
AIS - very high mag.
Case - biopsy
- Endocervical adenocarcinoma in situ --- intermed mag.jpg
AIS - intermed. mag.
- Endocervical adenocarcinoma in situ --- high mag.jpg
AIS - high mag.
- Endocervical adenocarcinoma in situ --- very high mag.jpg
AIS - very high mag.
- Endocervical adenocarcinoma in situ - alt --- intermed mag.jpg
AIS - intermed. mag.
- Endocervical adenocarcinoma in situ - alt --- high mag.jpg
AIS - high mag.
- Endocervical adenocarcinoma in situ - alt --- very high mag.jpg
AIS - very high mag.
- Endocervical adenocarcinoma in situ - p16 --- intermed mag.jpg
AIS - p16 - intermed. mag.
- Endocervical adenocarcinoma in situ - p16 --- high mag.jpg
AIS - p16 - high mag.
- Endocervical adenocarcinoma in situ - p16 --- very high mag.jpg
AIS - p16 - very high mag.
- Endocervical adenocarcinoma in situ - ki67 --- intermed mag.jpg
AIS - Ki-67 - intermed. mag.
- Endocervical adenocarcinoma in situ - ki67 --- high mag.jpg
AIS - Ki-67 - high mag.
- Endocervical adenocarcinoma in situ - ki67 --- very high mag.jpg
AIS - Ki-67 - very high mag.
www
- Endocervical AIS adjacent to normal (flickr.com/euthman).
- Endocervical adenocarcinoma in situ (techriver.net).
- Endocervical adenocarcinoma in situ (womenshealthsection.com).[4]
- Endocervical adenocarcinoma in situ - cytology (techriver.net).
{kind=link}
IHC
- p16 +ve.
- CEA +ve.
- Vimentin -ve.
Sign out
UTERINE CERVIX, BIOPSY: - HIGH-GRADE SQUAMOUS INTRAEPITHELIAL LESION (HSIL). - ENDOCERVICAL ADENOCARCINOMA IN SITU (AIS). - ACUTE AND CHRONIC INFLAMMATION. COMMENT: A p16 immunostain marks the full thickness of the squamous epithelium and is strong. A Ki-67 immunostain marks increased numbers of superficial squamous cells. The atypical endocervical epithelium (interpreted as AIS) is strongly p16 positive and has an increased proliferative activity with Ki-67 staining.
Micro
The atypical endocervical epithelium (interpreted as AIS) shows marked hyperchromasia, nuclear crowding and moderate nuclear atypia with a relatively abundant cytoplasm ( nucleus to cell size = 1:2 ).
See also
References
- ↑ Zaino, RJ. (Mar 2000). "Glandular lesions of the uterine cervix.". Mod Pathol 13 (3): 261-74. doi:10.1038/modpathol.3880047. PMID 10757337. http://www.nature.com/modpathol/journal/v13/n3/full/3880047a.html.
- ↑ Ioffe OB, Sagae S, Moritani S, Dahmoush L, Chen TT, Silverberg SG. (2003). "Proposal of a new scoring scheme for the diagnosis of noninvasive endocervical glandular lesions". Am J Surg Pathol 27 (4): 452–460. PMID 12657929.
- ↑ Nucci, Marisa R.; Oliva, Esther (2009). Gynecologic Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 167. ISBN 978-0443069208.
- ↑ URL: http://www.womenshealthsection.com/content/print.php3?title=gynpc006&cat=60&lng=english. Accessed on: 20 March 2013.