Difference between revisions of "Angiocentric glioma"
Jump to navigation
Jump to search
Jensflorian (talk | contribs) (more images added) |
Jensflorian (talk | contribs) m (wikify) |
||
| Line 9: | Line 9: | ||
| LMDDx = [[astrocytoma]], [[ependymoma]]. | | LMDDx = [[astrocytoma]], [[ependymoma]]. | ||
| Stains = | | Stains = | ||
| IHC = GFAP +/-ve, EMA +/-ve. | | IHC = GFAP +/-ve, [[EMA]] +/-ve. | ||
| EM = | | EM = | ||
| Molecular = | | Molecular = | ||
| Line 53: | Line 53: | ||
*Low cellularity and rich myxoid background- when compared to classical astrocytomas. | *Low cellularity and rich myxoid background- when compared to classical astrocytomas. | ||
**Mitotic activity may lead to eroneous diagnosis of [[anaplastic astrocytoma]]. | **Mitotic activity may lead to eroneous diagnosis of [[anaplastic astrocytoma]]. | ||
*Variably GFAP, EMA and S-100 positive | *Variably GFAP, [[EMA]] and S-100 positive | ||
* No IDH1/2 mutations. <ref>{{Cite journal | last1 = Raghunathan | first1 = A. | last2 = Olar | first2 = A. | last3 = Vogel | first3 = H. | last4 = Parker | first4 = JR. | last5 = Coventry | first5 = SC. | last6 = Debski | first6 = R. | last7 = Albarracin | first7 = CT. | last8 = Aldape | first8 = KD. | last9 = Cahill | first9 = DP. | title = Isocitrate dehydrogenase 1 R132H mutation is not detected in angiocentric glioma. | journal = Ann Diagn Pathol | volume = 16 | issue = 4 | pages = 255-9 | month = Aug | year = 2012 | doi = 10.1016/j.anndiagpath.2011.11.003 | PMID = 22445362 }}</ref> | * No IDH1/2 mutations. <ref>{{Cite journal | last1 = Raghunathan | first1 = A. | last2 = Olar | first2 = A. | last3 = Vogel | first3 = H. | last4 = Parker | first4 = JR. | last5 = Coventry | first5 = SC. | last6 = Debski | first6 = R. | last7 = Albarracin | first7 = CT. | last8 = Aldape | first8 = KD. | last9 = Cahill | first9 = DP. | title = Isocitrate dehydrogenase 1 R132H mutation is not detected in angiocentric glioma. | journal = Ann Diagn Pathol | volume = 16 | issue = 4 | pages = 255-9 | month = Aug | year = 2012 | doi = 10.1016/j.anndiagpath.2011.11.003 | PMID = 22445362 }}</ref> | ||
*MIB-1 between 1-5% | *MIB-1 between 1-5% | ||
| Line 74: | Line 74: | ||
Image:Neuropathology_case_V_03.jpg | Angiocentric glioma - high mag. (WC/jensflorian) | Image:Neuropathology_case_V_03.jpg | Angiocentric glioma - high mag. (WC/jensflorian) | ||
Image:Neuropathology_case_V_04.jpg | Angiocentric glioma - GFAP immunostain (WC/jensflorian) | Image:Neuropathology_case_V_04.jpg | Angiocentric glioma - GFAP immunostain (WC/jensflorian) | ||
Image:Neuropathology_case_V_05.jpg | Angiocentric glioma - EMA immunostain (WC/jensflorian) | Image:Neuropathology_case_V_05.jpg | Angiocentric glioma - [[EMA]] immunostain (WC/jensflorian) | ||
Image:Neuropathology_case_V_06.jpg | Angiocentric glioma - MAP2 immunostain (WC/jensflorian) | Image:Neuropathology_case_V_06.jpg | Angiocentric glioma - MAP2 immunostain (WC/jensflorian) | ||
Image:Neuropathology_case_V_07.jpg | Angiocentric glioma - MIB-1 immunostain (WC/jensflorian) | Image:Neuropathology_case_V_07.jpg | Angiocentric glioma - MIB-1 immunostain (WC/jensflorian) | ||
Revision as of 10:52, 23 September 2015
| Angiocentric glioma | |
|---|---|
| Diagnosis in short | |
 Angiocentric glioma. H&E stain. | |
| LM DDx | astrocytoma, ependymoma. |
| IHC | GFAP +/-ve, EMA +/-ve. |
| Gross | enlargened gyri |
| Site | brain - usu. grey matter |
|
| |
| Clinical history | epilepsy-associated |
| Prevalence | very rare - no age prevalence |
| Prognosis | good (WHO Grade I) |
Angiocentric glioma, is a WHO grade I glioma. It is super rare.
General
- previously called monomorphic angiocentric glioma or angiocentric neuroepithelial tumour.
- Own entity introduced in the WHO 2007 classification.[1]
- Low-grade glioma - WHO Grade I by definition, but a single recurrence with anaplastic features has been described.[2]
- Classically a non-enhancing, superficial cerebrocortical lesion.
- Associated with epilepsy.
- No association with any tumour syndromes.
Gross
- Usually well-circumscribed.
- Enlargement of cortex possible.
Microscopic
Features:
- Monommorphic, bipolar, spindled cells around blood vessels.
- mimicking ependymal pseudorosettes (DD: ependymoma).
- Solid growth with palisaded arrays possible.
- Low cellularity and rich myxoid background- when compared to classical astrocytomas.
- Mitotic activity may lead to eroneous diagnosis of anaplastic astrocytoma.
- Variably GFAP, EMA and S-100 positive
- No IDH1/2 mutations. [3]
- MIB-1 between 1-5%
DDx of angiocentric glioma (brief):
Molecular
- Deletion-truncation breakpoints in MYB/MYBL on 6q23-[4]
Images
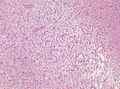
Angiocentric glioma - low mag. (WC/jensflorian)
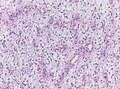
Angiocentric glioma - intermed mag. (WC/jensflorian)
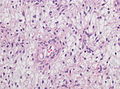
Angiocentric glioma - high mag. (WC/jensflorian)
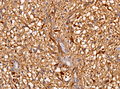
Angiocentric glioma - GFAP immunostain (WC/jensflorian)
Angiocentric glioma - EMA immunostain (WC/jensflorian)

Angiocentric glioma - MAP2 immunostain (WC/jensflorian)

Angiocentric glioma - MIB-1 immunostain (WC/jensflorian)






See also
References
- ↑ Brat, DJ.; Scheithauer, BW.; Fuller, GN.; Tihan, T. (Jul 2007). "Newly codified glial neoplasms of the 2007 WHO Classification of Tumours of the Central Nervous System: angiocentric glioma, pilomyxoid astrocytoma and pituicytoma.". Brain Pathol 17 (3): 319-24. doi:10.1111/j.1750-3639.2007.00082.x. PMID 17598825.
- ↑ Wang, M.; Tihan, T.; Rojiani, AM.; Bodhireddy, SR.; Prayson, RA.; Iacuone, JJ.; Alles, AJ.; Donahue, DJ. et al. (Oct 2005). "Monomorphous angiocentric glioma: a distinctive epileptogenic neoplasm with features of infiltrating astrocytoma and ependymoma.". J Neuropathol Exp Neurol 64 (10): 875-81. PMID 16215459.
- ↑ Raghunathan, A.; Olar, A.; Vogel, H.; Parker, JR.; Coventry, SC.; Debski, R.; Albarracin, CT.; Aldape, KD. et al. (Aug 2012). "Isocitrate dehydrogenase 1 R132H mutation is not detected in angiocentric glioma.". Ann Diagn Pathol 16 (4): 255-9. doi:10.1016/j.anndiagpath.2011.11.003. PMID 22445362.
- ↑ Ramkissoon, LA.; Horowitz, PM.; Craig, JM.; Ramkissoon, SH.; Rich, BE.; Schumacher, SE.; McKenna, A.; Lawrence, MS. et al. (May 2013). "Genomic analysis of diffuse pediatric low-grade gliomas identifies recurrent oncogenic truncating rearrangements in the transcription factor MYBL1.". Proc Natl Acad Sci U S A 110 (20): 8188-93. doi:10.1073/pnas.1300252110. PMID 23633565.